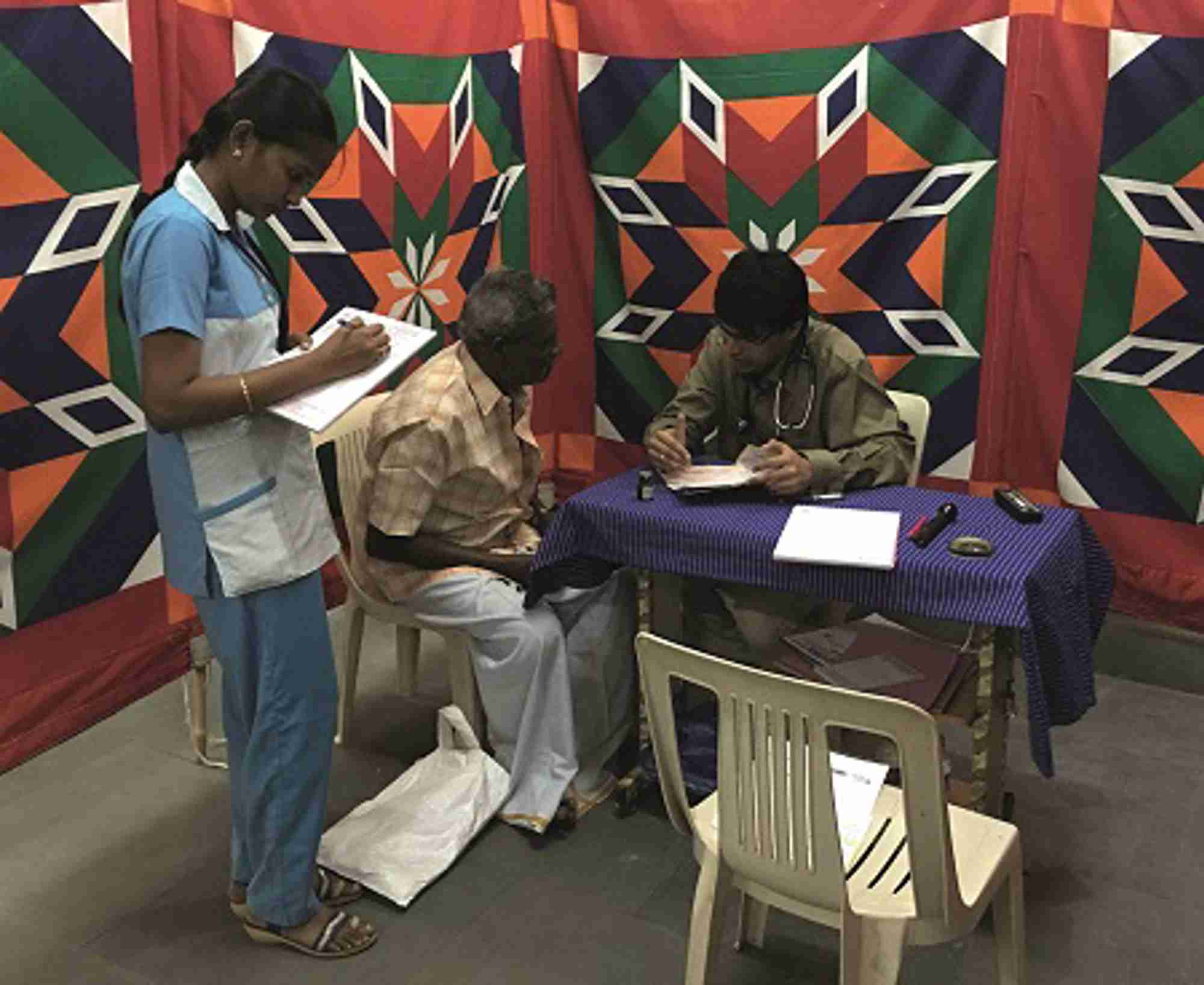
Figure 1. Diabetes and thyroid screening camps are an important facet of private healthcare in India
The Indian and British undergraduate medical education and training systems share a lot of similarities. Postgraduate specialty endocrinology training in India is highly competitive. As of 2015, there were 31 hospitals with accredited endocrine teaching programmes.1 Many Indian graduates therefore travel overseas to the UK and USA in pursuit of specialty training. The presence of a diverse ethnic Indian population in the UK, excellent postgraduate training opportunities and prospects for consultant jobs attract Indian doctors to the multicultural and multi-ethnic NHS.
We were attracted to the UK by this Western education and a hope of specialist training and long term prospects. Both of us ascended the ladder in the NHS, from senior house officer in medicine to clinical fellow, speciality registrar and clinical research associate in endocrinology over a period spanning more than 10 golden years. We witnessed the Callman training system and foundation programmes, and competed with the best for perfect specialty endocrine training.
After understanding the nuances of working in the NHS, we were all set to step up to a consultant post. However, our family situations beckoned us back to India. This was the beginning of a new path and chapter in our lives. We were both apprehensive about returning to India, as the system of endocrine practice there differs in many ways from that in the UK.
We will take advantage of our experience to attempt to analyse the major differences in the pattern of disorders, healthcare facilities, delivery of care and clinical training in endocrinology in India when compared with the UK. In addition, we will provide a brief overview of healthcare models worldwide, to aid understanding of how different healthcare models affect the delivery of endocrine care in India.
INDIAN HEALTHCARE MODELS
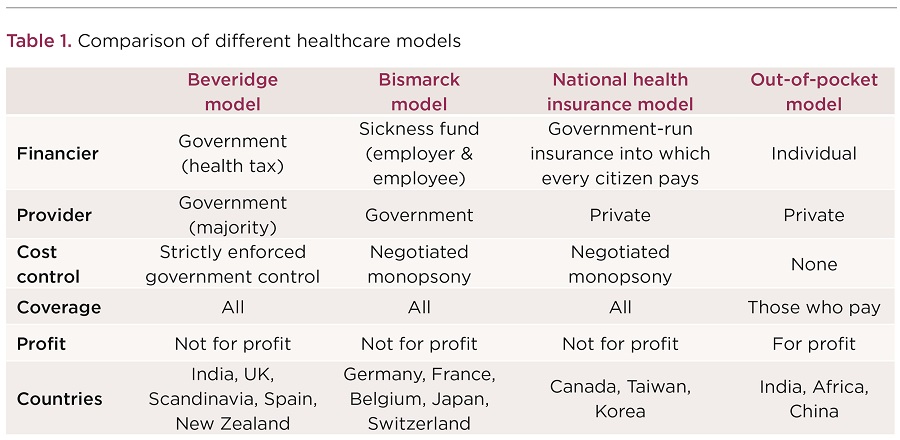
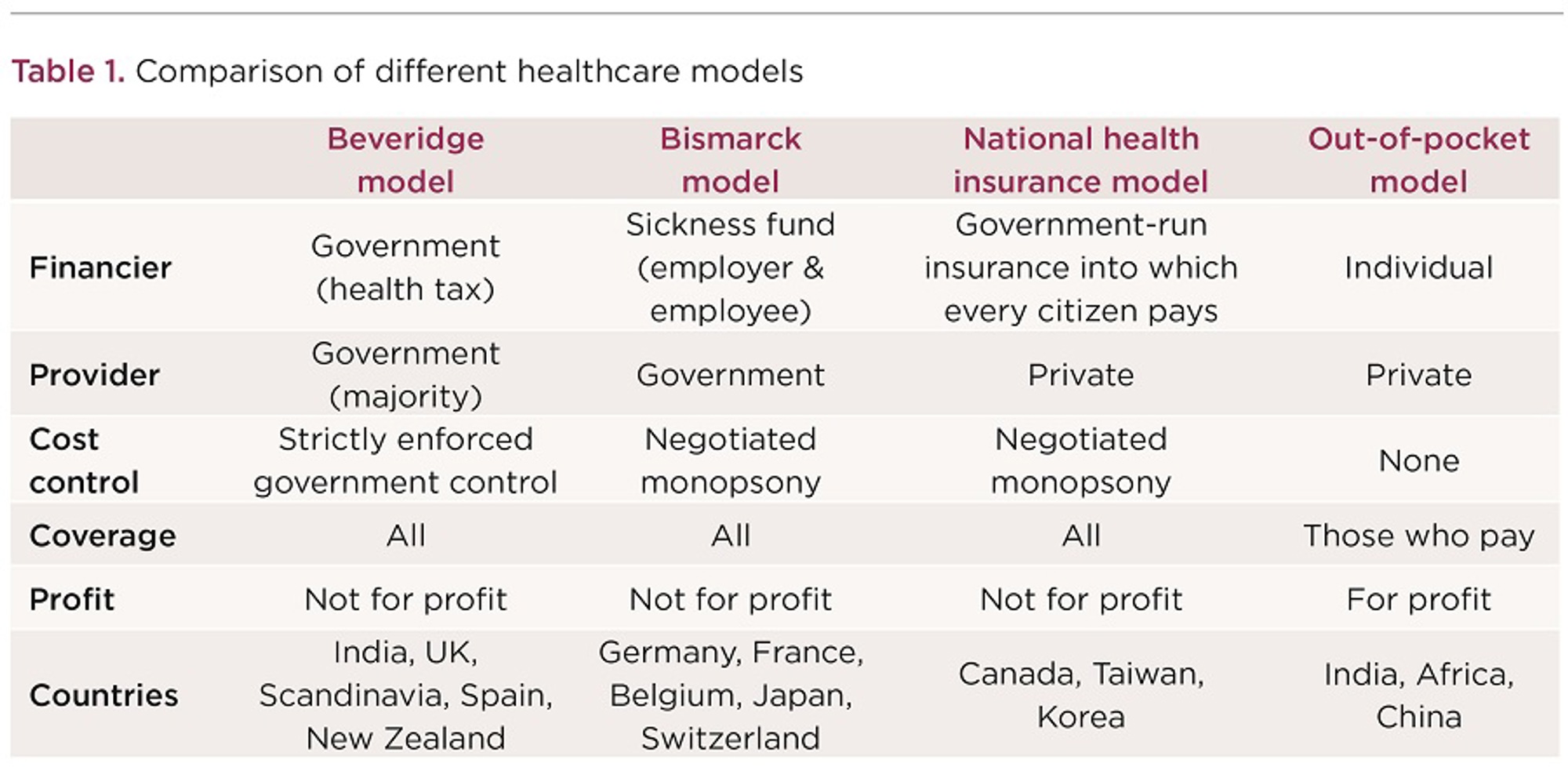
Around the globe, you will find four major models of healthcare:2
- Beveridge
- Bismarck
- national health insurance
- out-of-pocket.
Table 1 (below) gives an overview of these models. The Indian healthcare model is a mixture of the Beveridge and out-of-pocket models. The Government/state-run hospitals (Beveridge) provide healthcare to all, but people from the lower and middle income strata of society are their main users. The upper middle and high income strata of society use private healthcare facilities (out-of-pocket), due to their better infrastructure. Private healthcare has a range of facilities from small clinics to tertiary level hospitals, and hence caters to the lower and middle income sectors too.
The corporate sector (tertiary private hospitals) has established chains of hospitals across India with world class, state-of-the-art facilities. Such chains often operate a ‘hub and spoke’ model, whereby their peripheral clinics feed into their secondary and tertiary care hospitals for higher levels of care. To give an indication of the scale at which the corporate sector hospitals operate in India, the Apollo hospital chain has more than 60 secondary and tertiary care hospitals employing about 47,000 employees, more than 150 primary care clinics, 115 telemedicine units and over 2,200 pharmacies across Asia.
'The luxuries of Indian endocrine private practice include the availability of state-of-the-art technology with an amazingly short waiting time'
The tertiary hospitals have telemedicine, teleradiology and tele-ICU (intensive care unit) facilities to connect to the remotest parts of India and neighbouring countries. Relatives and friends of patients in ICU can see and communicate with their loved ones from anywhere in the world. For a country as big as India, such technologies are transforming the way healthcare is delivered to every nook and corner of the country.
These facilities, along with the comparatively cheap healthcare costs and quicker access to healthcare, attract people from other countries, leading to the development of so-called ‘medical tourism’ in India.
INDIAN ENDOCRINE PRIVATE HEALTH CLINICS
The luxuries of Indian endocrine private practice include the availability of state-of-the art technology with an amazingly short waiting time. The waiting time for magnetic resonance imaging (MRI) or positron emission tomography (PET) scanning is generally less than 24 hours, and an insulin pump or ablative radioiodine therapy could be scheduled within 48 hours.
However, the entire cost has to be borne by the patient, including outpatient consultations, investigations and therapies such as medications. Inpatient costs can be claimed through various private insurance companies. The stark differences between the NHS and the Indian private clinics include the challenge and skill of assessing the economic capacity of the patient and of choosing the most important investigatory modalities and ideal cost-effective remedies. The capacities of patients seeking consultations to pay could vary from the super-rich to the most economically challenged.
India is the diabetes capital of the world and, in a country of more than one billion people, the endocrine and diabetes clinics are over-crowded. In the UK, if a single registrar sees 25 outpatients per day, it is considered a huge number. As private endocrinologists in India, we each see an average of 50 outpatients; this number could, at times, be as high as 90 endocrine/diabetes patients. The working schedule is also variable, with evening clinics running up to 10.00pm.
Although sometimes tiring, the clinics are very challenging and stimulating. The icing on the cake is that we generally only see diabetes and endocrine patients and the general medicine commitment is negligible.

Figure 2. Diabetes prevention workshops for the general public are organised by private clnics
Most private hospitals are equipped with an operating theatre, an in-house pharmacy and a comprehensive laboratory. The endocrine private clinics cater to walk-in patients who include self-referrals and referrals from other doctors.
The establishment of a private endocrine clinic is quite challenging, reminiscent of a DIY self-assembly project. The training curriculum to become a specialty registrar didn’t include investing money for private clinic infrastructure, planning the locality of a practice, acquiring bank loans, or shortlisting laboratory and hospital equipment. The silver lining is the support offered by family and friends.
Shortlisting, employing and training nurses and dieticians who have no experience in specialty medicine, as well as recruiting laboratory personnel, support staff, hospital managers and receptionists, test our management skills to the core.
Another important facet of private healthcare in India includes diabetes and thyroid screening camps (Figure 1), organised in semi-urban and rural areas at regular intervals, free of cost. These serve the dual purpose of educating the public about non-communicable diseases and also estimating the disease burden in various sections of the community. Private clinics also undertake other social welfare schemes, including developing diabetes prevention strategies by educating school children and the general public (Figure 2). Organisation of these activities requires a lot of co-ordination and adaptation to the community setting, and leadership skills are put to the test.
PATTERNS OF INDIAN ENDOCRINE DISORDERS
Given the differences in genetic background, diet, lifestyle, and environmental factors between the West and the East, one might expect variation in the pattern of diseases between the UK and India.
'As a private endocrinologist in India, we each see an average of 50 outpatients per day; this number could be as high as 90'
Following the elimination of iodine deficiency disorders through mandatory iodination programmes, the most common cause of thyroid disorders in India now is autoimmunity. On the other hand, infiltrative disorders of the adrenal gland, especially tuberculosis and histoplasmosis, contribute to significant numbers of cases of primary adrenal insufficiency. Studies have shown that about 46–56% of patients with clinical tuberculosis have adrenal insufficiency.3 Unlike patients with Addison’s disease, a significant proportion of those with infiltrative diseases recover their adrenal function after medical treatment.
There is a high prevalence of Sheehan’s syndrome (postpartum hypopituitarism), which is often under-diagnosed. In certain parts of India, such as Kashmir, where there is a higher rate of home deliveries and maternal anaemia, the prevalence is as high as 3% of all deliveries in women above the age of 20 years.4 Certain causes of hypopituitarism are unique to the East: the bite of the Russell’s viper (Daboia russelii russelii) is an uncommon, but important, cause of the condition. The venom is vasculotoxic and contains procoagulant enzymes that activate clotting factors, eventually leading to disseminated intravascular coagulation5 and hypopituitarism, which is a recognised complication. Tuberculosis is another important cause of hypopituitarism.
Among metabolic bone diseases, certain conditions, such as fluorosis and oncogenic osteomalacia, contribute to significant morbidity and are seen more often in the East.
By combining the clinical acumen acquired during our training in the UK with state-of-the art facilities in the corporate sector hospitals, we have ventured into managing challenging clinical cases with newer modalities of treatment, such as robotic surgery for selected cases of endocrine tumours.6
IN SUMMARY
The diversity of clinical presentations and rare diagnoses is indeed mind-boggling. They keep us on our toes and prompt us to glance again at textbooks or call consultant colleagues and friends in the UK. This interaction has helped scientific camaraderie, and we continue to maintain links with our mentors and supervising consultants from the UK. Academic exchanges have been mutually rewarding, with the identification of rare disorders, novel mutations and many joint publications.7–9
Looking back, we appreciate that our current roles fulfil an important aspect of providing holistic endocrine and diabetes care and also interconnect scientific opportunities between two different systems of healthcare. We, as British-trained Indian endocrinologists, continue to ‘Mind the Gap’ in our Indian practice, and keep looking forward to fantastic opportunities to collaborate and advance the science of endocrinology with our friends and colleagues from the UK.
Anand K Annamalai, Ashwin Speciality Hospital, Madurai, Tamil Nadu, India
Narayanan Kandasamy, Apollo Hospital, Chennai, Tamil Nadu, India
REFERENCES
1. Bajaj S et al. 2015 Indian Journal of Endocrinology & Metabolism 19 448–450.
2. Wallace LS 2013 Annals of Family Medicine 11 84.
3. Prasad GA et al. 2000 Indian Journal of Chest Diseases & Allied Sciences 42 83–93.
4. Zargar AH et al. 2005 Fertility & Sterility 84 523–528.
5. Mukherjee AK 2008 Toxicon 51 923–933.
6. Ragavan N et al. 2016 Journal of Robotic Surgery 10 373–374.
7. Annamalai AK et al. 2016 Journal of Clinical Endocrinology & Metabolism 101 390–393.
8. Justin C et al. 2013 QJM 106 1123–1125.
9. Kandasamy N et al. 2014 Proceedings of the National Academy of Sciences of the USA 111 3608–3613.


{kind=link}
{kind=link}