Obesity is commonly defined as a body mass index (BMI) ≥30kg/m2. Lower cut-offs are used in high-risk groups, such as South Asian, Chinese, Arab and Black populations. It is a long-term metabolic disease that exerts a substantial but modifiable influence on cardiovascular disease (CVD).1
Obesity confers increased CVD risk in a multimodal fashion by its association with established CVD risk factors including hypertension, dyslipidaemia and insulin resistance.1 It is also now increasingly clear that obesity itself independently contributes to coronary artery disease (CAD) and heart failure.1,2
PATHOPHYSIOLOGICAL PATHWAYS LINKING OBESITY TO CAD
'Epidemiological data consistently show a higher incidence of heart failure among people with obesity, even when accounting for traditional risk factors.'
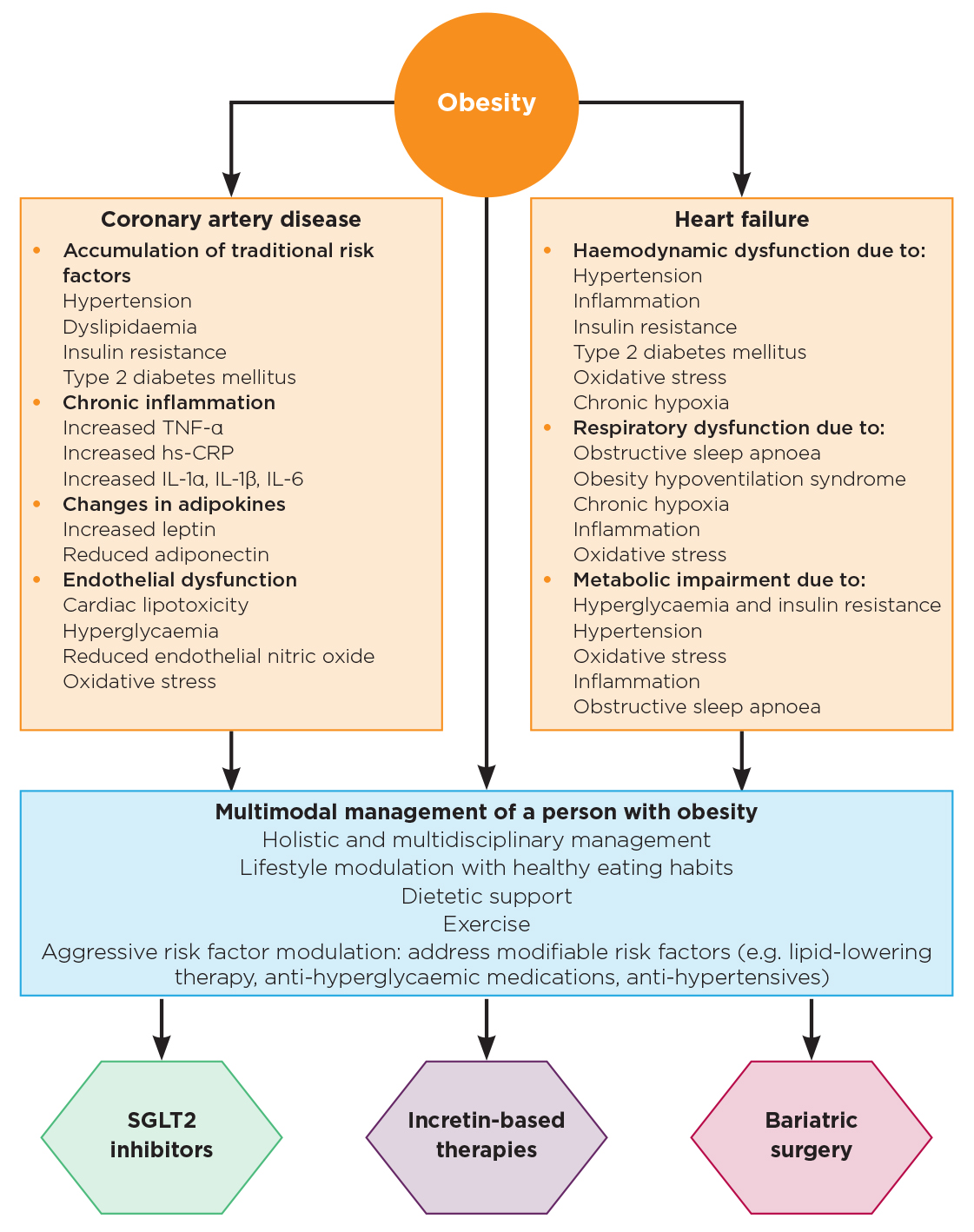
Obesity is associated with pathological alterations in systemic and vascular inflammation, adipokines, insulin resistance, lipids and endothelial function (Figure). Individuals with obesity typically demonstrate a chronic pro-inflammatory profile, with elevations in tumour necrosis factor-α, high-sensitivity C-reactive protein and interleukins including IL-1α, IL-1β and IL-6.1,3 These cytokines contribute to endothelial dysfunction, oxidative injury and macrophage lipid accumulation within arterial walls.1
Obesity-related adipokine changes with increases in leptin (pro-inflammatory) and reductions in adiponectin (anti-inflammatory) have also been demonstrated to increase the risk of CAD.1 Furthermore, by worsening insulin resistance, with a consequent excess of advanced glycation end products and reactive oxygen species, excess delivery of fatty acids to the myocardium (cardiac lipotoxicity) and endothelial dysfunction, obesity markedly increases the risk of atherosclerosis and CAD.1
OBESITY AND HEART FAILURE
Epidemiological data consistently show a higher incidence of heart failure among people with obesity, even when accounting for traditional risk factors. Progressive elevations in BMI correspond to higher risk of heart failure in a graded manner.
Clinically, this risk expresses itself most clearly in heart failure with preserved ejection fraction (HFpEF). Patients typically demonstrate a combination of increased left-ventricular (LV) wall thickness, impaired diastolic filling, reduced natriuretic peptide release and elevated pulmonary pressures during exertion.
These abnormalities translate into reduced exercise tolerance and symptom burden disproportional to structural findings. Additionally, obesity-prevalent respiratory conditions, such as obesity hypoventilation syndrome and obstructive sleep apnoea, compound the pathology by amplifying sympathetic drive, promoting intermittent hypoxia and increasing haemodynamic load.1,4
THE OBESITY PARADOX: METHODOLOGICAL ARTEFACT
Although obesity clearly contributes to the pathogenesis of heart failure, some studies have suggested that higher BMI may be associated with improved survival, once heart failure is established: the so-called ‘obesity paradox’.5
Closer examination, however, indicates that these findings are prone to methodological bias. Frailty and unintentional weight loss disproportionately affect individuals with lower BMI, while treatment patterns often differ across weight categories. A study incorporating more detailed anthropometric measures of visceral obesity (waist-to-height ratio), rather than solely BMI, demonstrated that any apparent survival advantage is attenuated in people with central obesity.6 Therefore, the ‘obesity paradox’ probably does not represent a true biological phenomenon, but rather reflects methodological limitations such as collider bias.7
THERAPEUTIC STRATEGIES: A CARDIOMETABOLIC APPROACH
Managing obesity in the context of CVD requires a broad, co-ordinated approach. Although dietary and behavioural interventions are essential foundations for weight management, durable success is difficult to achieve without additional therapeutic support, particularly in those with significant or long-standing obesity.8
Medical management options

A summary of the key pathogenic mechanisms by which obesity increases the risk of both coronary artery disease and heart failure. Also demonstrated are the key therapeutic considerations for managing a patient with obesity, to prevent adverse cardiovascular conditions in those without established cardiovascular disease and to improve outcomes in those with pre-existing cardiovascular disease. hs-CRP, high-sensitivity C-reactive protein; TNF-α, tumour necrosis factor-α.
In recent years, pharmacotherapy has become an increasingly important component of cardiometabolic care. Sodium–glucose cotransporter-2 (SGLT2) inhibitors, for example, provide consistent reductions in heart failure hospitalisations and cardiovascular mortality – benefits that appear across BMI categories and are not solely attributable to weight loss.1 These therapies modulate renal sodium handling, improve circulatory efficiency and confer metabolic advantages that contribute to their cardiovascular effects.1
Glucagon-like peptide-1 receptor agonists (GLP1-RAs) have demonstrated substantial weight-loss efficacy alongside favourable cardiovascular risk factor modulation.1 Emerging data in obesity-related HFpEF suggest improvements in symptoms, exercise capacity, inflammatory markers and mortality.1,9 Dual incretin agonists also show promise and may provide even greater CVD risk reduction,10,11 although long-term data are awaited.
Bariatric surgery for cardiometabolic disease
For individuals with severe obesity, bariatric surgery remains the most effective long-term strategy for achieving significant weight reduction. Beyond weight loss, improvements have been observed in LV mass, diastolic performance, endothelial function, inflammation, lipid transport and multiple cardiometabolic risk factors, with demonstrable reductions in CVD mortality.1,12
However, individuals with CAD or heart failure require thorough cardiovascular evaluation and careful perioperative planning. Procedures with lower physiological demand, such as sleeve gastrectomy, may be preferable in those with advanced cardiac disease.1
CONCLUSION
Obesity is a complex, multisystem disease that plays a critical role in the development and progression of CAD and heart failure. Recognising obesity as a primary driver of CVD reinforces the need for early, proactive intervention. Treatment of obesity (both medical and surgical) can potentially alter the pathological trajectory from excess adiposity to cardiovascular failure.
SAFWAAN ADAM
Consultant Endocrinologist and Honorary Senior Lecturer, Christie NHS Foundation Trust, University of Manchester, and NIHR Biomedical Research Centre, Manchester
AKHEEL A SYED
Consultant Endocrinologist and Honorary Professor, Salford Royal Hospital, Northern Care Alliance NHS Foundation Trust, and University of Manchester
REFERENCES
1. Syed AA et al. 2025 Heart Failure Clinics https://doi.org/10.1016/j.hfc.2024.12.006.
2. Powell-Wiley TM et al. 2021 Circulation https://doi.org/10.1161/cir.0000000000000973.
3. Adam S et al. 2019 Diabetes & Vascular Disease Research https://doi.org/10.1177/1479164119826479.
4. Bjork S et al. 2024 Sleep Medicine Clinics https://doi.org/10.1016/j.jsmc.2024.02.009.
5. Lavie CJ et al. 2003 American Journal of Cardiology https://doi.org/10.1016/s0002-9149(03)00031-6.
6. Butt JH et al. 2023 European Heart Journal https://doi.org/10.1093/eurheartj/ehad083.
7. Holmberg MJ & Andersen LW 2022 JAMA https://doi.org/10.1001/jama.2022.1820.
8. Lopez-Jimenez F et al. 2022 European Journal of Preventive Cardiology https://doi.org/10.1093/eurjpc/zwac187.
9. Duhan S et al. 2025 International Journal of Cardiology https://doi.org/10.1016/j.ijcard.2025.133604.
10. Packer M et al. 2025 New England Journal of Medicine https://doi.org/10.1056/NEJMoa2410027.
11. Mamas MA et al. 2025 European Heart Journal Open https://doi.org/10.1093/ehjopen/oeaf117.
12. Adam S et al. 2022 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/clinem/dgac244.

{kind=link}