With advancements in early cancer detection and improved therapies, the population of cancer survivors continues to grow significantly. In the UK alone, approximately 385,000 new cancer cases are diagnosed annually. Remarkably, about half of individuals diagnosed with cancer now survive for at least 10 years post-diagnosis.1 However, extended survival brings a series of chronic health issues, prominently including an increased risk of bone fractures.
Fractures in cancer survivors significantly impact quality of life and healthcare resources and are associated with increased mortality.2 Bone health in oncology patients is therefore one of the three research sub-themes within the Manchester Biomedical Research Centre (BRC) Living With and Beyond Cancer Theme, led by Claire Higham.
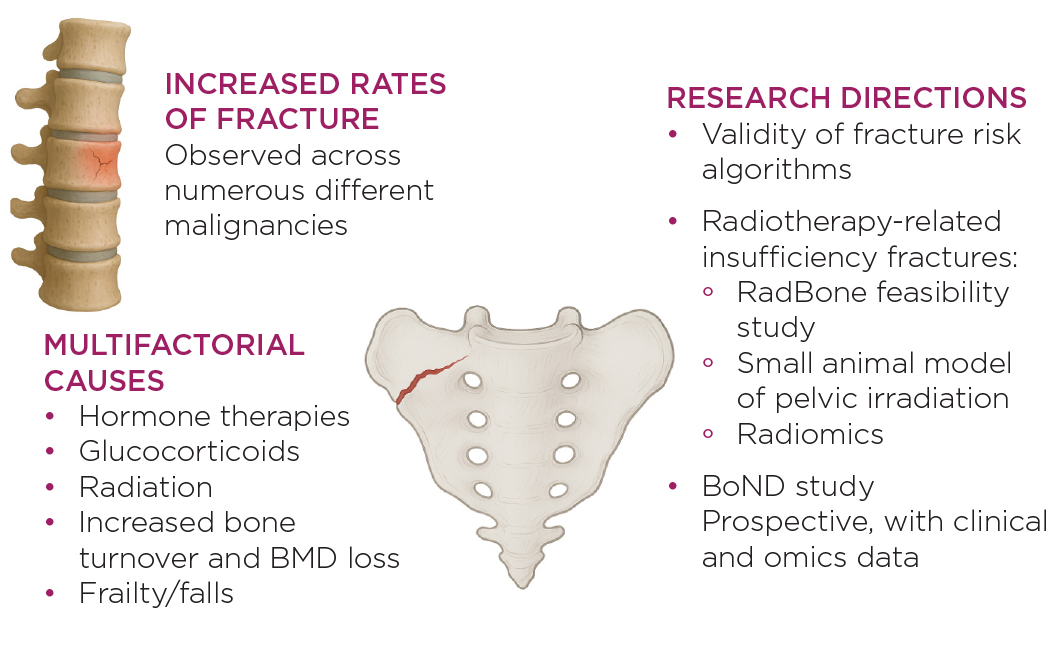
A recent UK population-based study using the Clinical Practice Research Datalink (CPRD) found that survivors of 15 out of the 20 most common adult cancers had a heightened risk of fractures. This risk persisted up to five years after diagnosis, with major osteoporotic fractures – of the hip, spine, pelvis, wrist and proximal humerus – being especially common across multiple tumour types.2

Bone health in oncology patients.
The underlying causes of cancer-related bone fragility are multifactorial. Cancer therapies, particularly hormone treatments and glucocorticoids, play a central role. In breast and prostate cancer, aromatase inhibitors, ovarian suppression and androgen deprivation therapy (ADT) significantly reduce sex steroid levels, leading to increased bone turnover and loss of bone mineral density (BMD).3 High-dose glucocorticoids, used in various oncological settings, further exacerbate bone resorption.4 These changes, compounded by age-related frailty and sarcopenia, increase the risk of falls and fractures.5
DETERMINING THE RISKS
Despite recognition of these risks, fracture prediction tools like FRAX® may not be as accurate in oncology populations. Recent data from trials such as STAMPEDE suggest the need for broader bone protective strategies beyond those guided by current risk thresholds.6 Building on this, our team at the University of Manchester is working to address key gaps in risk stratification and management.
As part of this work, we are exploring the validity of fracture risk algorithms in 500,000 adult oncology patients using UK CPRD data, in collaboration with Darren Ashcroft at the NIHR Patient Safety Research Centre. Our goal is to assess how well current tools identify patients who go on to fracture, particularly those with limited life expectancy or who are undergoing specific cancer therapies.
A second focus is radiotherapy-related insufficiency fractures (RRIFs), which represent a distinct clinical entity most commonly seen after pelvic radiotherapy. These fractures often occur even in patients with normal BMD, indicating that traditional tools may miss this risk. While best practice guidance from the Pelvic Radiation Disease Association (PRDA) exists, it is not evidence-based.7 To address this, we recently completed a feasibility study (RadBone), funded by an MRC Clinical Academic Research Partnership (Claire Higham), at the Christie Hospital in Manchester.8 This study piloted a musculoskeletal health programme combining physical assessment, exercise prehabilitation, fracture risk evaluation and targeted bone treatments. Results are expected in 2025 and will inform a future UK multicentre clinical intervention trial.
UNDERLYING MECHANISMS
Complementing this clinical research, we are also investigating the mechanistic underpinnings of RRIFs through a University of Manchester MRC-funded PhD project (Victoria Chatzimavridou Grigoriadou). In collaboration with the University of Sheffield SkeletAL Lab, we are developing a small animal model of pelvic radiotherapy to explore bone structure, turnover and microdamage using imaging and histomorphometry techniques. This work aims to characterise how radiation affects different bone compartments, including trabecular and cortical regions. Novel radiomic techniques and detailed analysis of RRIFs are also being taken forward as a BRC-funded physics-based PhD at the University of Manchester (Artemis Bouzaki).
In parallel, we have launched the Bone Health in Oncology Dataset (BOnD) within our BRC theme. This prospective study is recruiting patients attending the Metabolic Bone Clinic at the Christie, incorporating clinical assessments, polygenic risk scores and omics profiling to better understand fracture susceptibility in cancer patients.
FRACTURES AND CANCER OUTCOMES
Fractures have a measurable and concerning impact on cancer outcomes. For example, men with prostate cancer receiving ADT who sustained skeletal fractures had reduced median survival compared with those without fractures.9 Similarly, fractures in patients with breast cancer have been linked to increased hospitalisation and mortality.10 A large Canadian registry study also reported that fracture-related mortality remains elevated for years after the initial event.11 These data underline the importance of targeted prevention strategies.
'Recent data from trials such as STAMPEDE suggest the need for broader bone protective strategies beyond those guided by current risk thresholds.'
The rising number of cancer survivors calls for a shift in how we view long-term care. While preventing recurrence remains a priority, we must also recognise and address survivorship-related complications, such as fragility fractures. Current guidelines offer practical approaches to fracture risk management, including BMD measurement, FRAX® assessment, and pharmacological treatments, such as bisphosphonates or denosumab. However, they may fall short in complex or rapidly evolving oncology settings.
There is growing momentum behind research into bespoke risk- prediction models and interventions that reflect cancer type, treatment history, co-morbidities and broader factors, such as frailty. Integrating fracture risk assessments into oncology care pathways, supported by clinician education and cross-disciplinary collaboration, will be vital.
Ultimately, supporting bone health in cancer survivors is not just about preventing fractures – it is about improving survival, maintaining independence and enhancing quality of life. With growing survivorship, recognising fractures as a preventable consequence of cancer and its treatment can help shape more holistic, proactive care.
CLAIRE E HIGHAM and VICTORIA CHATZIMAVRIDOU GRIGORIADOU
Department of Endocrinology, Christie Hospital NHS Foundation Trust; Division of Cancer Sciences, University of Manchester
The BOnD study and CPRD fracture risk work are being delivered through the NIHR Manchester BRC (NIHR203308). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. This work is also supported by the MRC (grant number MR/T024887/1; fellowship number MR/Z504166/1).
REFERENCES
1. Cancer Research UK 2024 Cancer Statistics for the UK https://www.cancerresearchuk.org/health-professional/cancer-statistics-for-the-uk.
2. Buzasi E et al. 2024 Lancet Healthy Longevity https://doi.org/10.1016/S2666-7568(23)00285-4.
3. Rachner TD et al. 2018 Lancet Diabetes & Endocrinology https://doi.org/10.1016/S2213-8587(18)30047-0.
4. Brown JE et al. 2020 Journal of Bone Oncology https://doi.org/10.1016/j.jbo.2020.100311.
5. Myint ZW et al. 2020 JAMA Network Open https://doi.org/10.1001/jamanetworkopen.2020.25826.
6. Jones C et al. 2023 Urology https://doi.org/10.1097/ju.0000000000003226.13.
7. PRDA 2022 Best Practice Pathway for Pelvic Radiation Disease https://www.prda.org.uk/wp-content/uploads/2022/09/PRDA_Best-Practice-Pathway_Toolkit.pdf.
8. Chatzimavridou Grigoriadou V et al. 2022 BMJ Open https://doi.org/10.1136/bmjopen-2021-056600.
9. Oefelein MG et al. 2002 Journal of Urology https://doi.org/10.1016/s0022-5347(05)64561-2.
10. Colzani E et al. 2016 British Journal of Cancer https://doi.org/10.1038/bjc.2016.314.
11. Ye C et al. 2022 Osteoporosis International https://doi.org/10.1007/s00198-022-06542-4.

{kind=link}