Adrenal tumours have become a familiar finding in endocrine practice, affecting 1–7% of adults. Some of these tumours can be cancerous, and up to half can produce hormones in excess, which is associated with increased cardiovascular, metabolic and mortality risks. Understanding how these risks arise, and how to stratify patients more precisely, remains a key challenge.
A new line of research is now exploring a surprising source of insight: the humble full blood count. By repurposing routine haematology results into inflammation-based scores, our group has uncovered systemic immune signatures linked to malignancy and hormonal activity in adrenal tumours.
HOW EXCESS ADRENAL HORMONES AFFECT THE IMMUNE SYSTEM
Cortisol, a key immunomodulator, exerts complex effects on immune function. Chronic excess, as seen in Cushing’s syndrome, is associated with characteristic haematological changes – neutrophilia, lymphopaenia and eosinopaenia – that increase susceptibility to infections. Even mild autonomous cortisol secretion (MACS), which lacks the classic signs of Cushing’s syndrome, appears to influence immune function in subtler, but still clinically relevant, ways. Similarly, catecholamines released by phaeochromocytomas can alter immune activation and inflammation, although the mechanisms remain less well defined.
INFLAMMATION-BASED SCORES: A WINDOW INTO SYSTEMIC INFLAMMATION
Inflammation-based scores have been proposed as surrogate markers of systemic inflammation in a range of conditions, such as ischaemic heart disease, stroke and cancer. These scores can easily be calculated using standard laboratory tests, such as full blood count and albumin, and correlate with acute and chronic inflammation.
The increasing interest in these markers is due to their recognised prognostic value as well as their cost-effectiveness, wide availability and practicality. For instance, an increase in the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio and systemic immuno-inflammation index (SII, the product of platelet count and NLR), and a decrease in the lymphocyte-to-monocyte ratio (LMR) and prognostic nutrition index (that considers serum albumin and the absolute lymphocyte count), reflect ineffective immune surveillance or an increased inflammatory state.
CORTISOL EXCESS AND INFLAMMATION-BASED SCORES
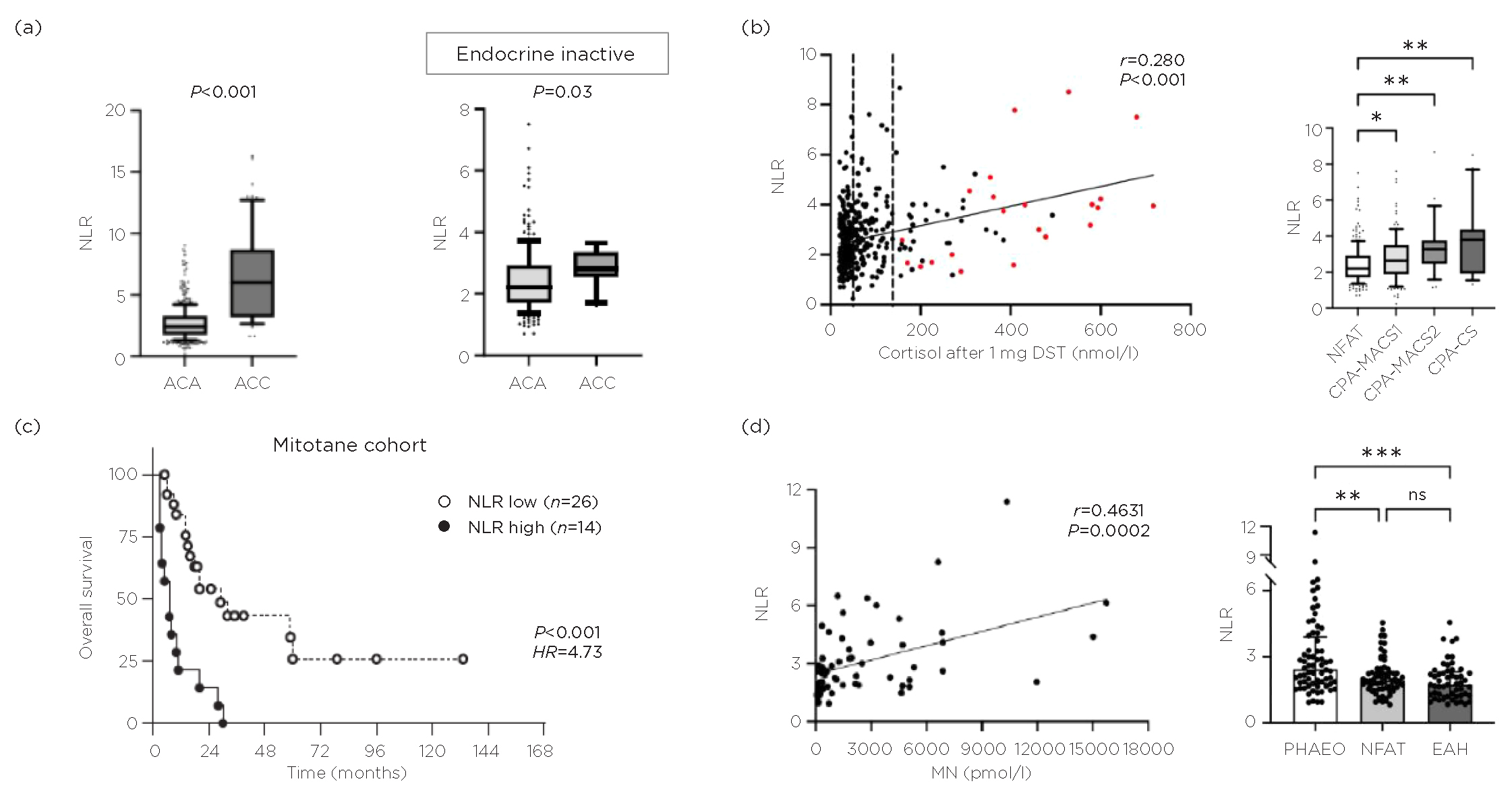
We recently explored how inflammation-based scores behave in benign adrenal tumours associated with cortisol excess. In a retrospective study of 375 patients, we found that NLR and SII rose in line with cortisol levels – across non-functioning adrenal tumours, MACS, and adrenal Cushing’s syndrome – while LMR decreased.1
These findings suggest that even modest cortisol excess disrupts immune cell populations and contributes to systemic inflammation. Importantly, this immune signature was detectable even in patients without overt features of Cushing’s syndrome. These changes may help explain the increased cardiometabolic burden associated with MACS and point toward potential uses for inflammation-based scores in risk stratification and monitoring.

(a) NLR in patients with adrenocortical adenomas (ACAs) versus ACCs. (b) NLR and cortisol secretion in patients with ACAs; MACS-1, possible MACS; MACS-2, definitive MACS; *P<0.05, **P<0.01 and ***P<0.001). (c) NLR and overall survival in patients with ACCs. (d) NLR and plasma metanephrines (MN) in patients with phaeochromocytomas (PHAEO) (EAH, essential hypertension; **P<0.002, ***P<0.0001). See footnote for acronyms and credits.
INSIGHTS FROM ADRENAL CANCER
Inflammation-based scores may also help distinguish benign from malignant adrenal tumours. In a cohort of patients with adrenocortical carcinomas (ACCs) or adrenocortical adenomas, we found significantly different inflammation-based scores in ACCs, even in those without hormone excess. This suggests that the malignancy itself contributes to systemic inflammation.2 In a separate study of 90 patients with advanced ACCs, an elevated NLR predicted earlier progression during mitotane treatment or systemic chemotherapy.3 These findings are now being validated in a multicentre study led by the European Network for the Study of Adrenal Tumors.
PHAEOCHROMOCYTOMAS: INFLAMMATION AND CATECHOLAMINES
Phaeochromocytomas also show evidence of systemic inflammation. We showed that affected patients had elevated preoperative NLR and SII values that correlated with plasma metanephrine levels.4 These scores improved after adrenalectomy or α-blockade, indicating a dynamic relationship between catecholamine excess and systemic inflammation.4
This is clinically important, as inflammation may contribute to the cardiovascular and metabolic complications observed in these patients. By better understanding this link, we may be able to optimise treatment strategies, not just for tumour control, but also to improve long-term outcomes.
CLINICAL TAKEAWAYS AND FUTURE DIRECTIONS
Inflammation-based scores offer a new, promising tool for assessing adrenal tumours. Their simplicity, broad availability and cost-effectiveness make them appealing for integration into routine care, especially when biochemical or imaging findings are inconclusive. They may help stratify cardiometabolic risk in MACS, monitor the systemic effects of adrenal hormone excess, understand how malignancy and hormone excess affect immune function, and predict prognosis in ACC.
CRISTINA L RONCHI
Reader in Endocrine Oncology, Department of Metabolism and Systems Science, College of Medicine and Health, University of Birmingham
ALESSANDRO PRETE
Clinical Associate Professor of Endocrinology, Department of Metabolism and Systems Science, College of Medicine and Health, University of Birmingham
REFERENCES
1. Favero V et al. 2023 European Journal of Endocrinology https://doi.org/10.1093/ejendo/lvad151.
2. Mangone A et al. 2025 Journal of Endocrinological Investigation https://doi.org/10.1007/s40618-024-02426-y.
3. Mangone A et al. 2023 Endocrine-Related Cancer https://doi.org/10.1530/ERC-22-0372.
4. Parazzoli C et al. 2025 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/clinem/dgae284.
FOOTNOTE
Acronyms: NFAT, non-functioning adrenal tumour; CPA, cortisol-producing adenoma; CS, Cushing’s syndrome; DST, dexamethasone-suppression test. Credits: Panels (a), (c) and (d) are reproduced from Mangone et al.,2 Mangone et al.3 and Parazzolo et al.4 respectively under a CC BY 4.0 licence.Panel (b) is reproduced from Favero et al.1 under a CC BY-NC 4.0 licence. All panels © The Authors.

{kind=link}