In 1978, Louise Joy Brown made history as the world’s first baby conceived through in vitro fertilisation (IVF) when she was born in Oldham, UK. The recent Netflix blockbuster ‘Joy’ vividly captures the spectrum of emotions that this breakthrough evoked, from fears of ‘Dr Frankenstein’ playing God, to celebrations of what many considered to be nothing short of a medical miracle.
'This convergence of the rich clinical data produced during the IVF process and advanced computational tools presents a unique opportunity to transform how we approach fertility treatment.'
Almost 50 years later, IVF is now an established treatment for infertility. Although NICE recommends up to three cycles of IVF for couples with infertility, there remains a ‘postcode lottery’, with additional local restrictions towards access. Thus, many couples must resort to private sector care, either if treatment is unsuccessful or if more than one child is desired to complete their family. Against this backdrop, there is great pressure on each IVF cycle to be successful, which has led to an industry that often welcomes early adoption of new technologies, albeit sometimes prematurely before the required testing has been conducted.
THE ROLE OF ARTIFICIAL INTELLIGENCE
Artificial intelligence (AI) has emerged as a potentially transformative breakthrough across medicine, but the AI revolution has particularly bloomed in the fertility sector. In 2014, there were only a dozen papers on AI in IVF treatment. By 2024, this had increased by more than 20-fold, speaking to its suitability to optimise many different aspects of the process.
In a parallel technological revolution, computational power has grown exponentially alongside sophisticated statistical methodologies, creating unprecedented opportunities for refined predictive capabilities through AI. This convergence of the rich clinical data produced during the IVF process and advanced computational tools presents a unique opportunity to transform how we approach fertility treatment.1

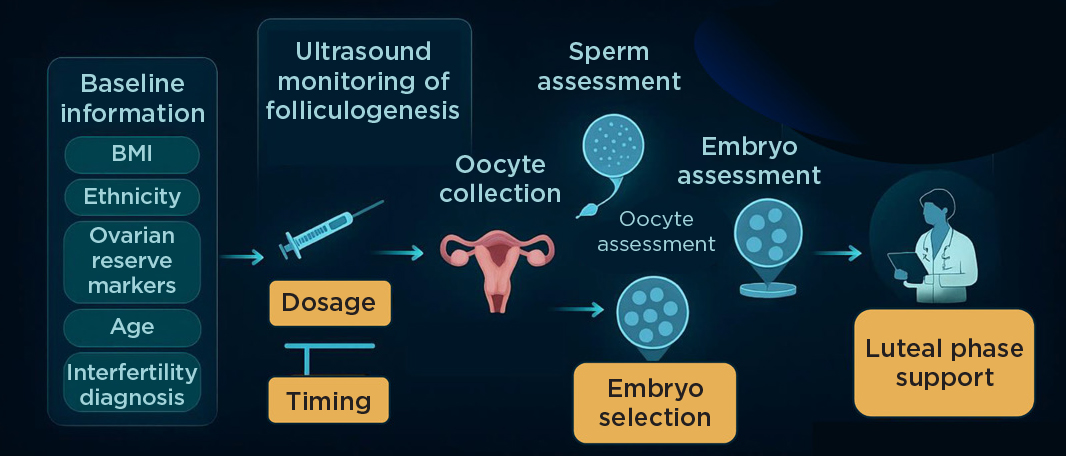
IVF and the utility of AI.
For some uses, AI offers capabilities beyond that of humans: for example, during time-lapse analysis of embryos, where AI can analyse days of footage to detect patterns imperceptible to the human eye, in order to predict embryo quality and the chance of genetic abnormality, without the need for invasive pre-implantation genetic testing. In others, AI can automate tasks that currently require expert clinician or embryologist input, freeing up their time to be redirected elsewhere, thus increasing capacity and reducing costs to meet an escalating demand for care.
THE ISSUE OF CLINICAL RESPONSIBILITY
AI encompasses a broad ecosystem of technologies, including machine learning (ML), robotics and computer vision. ML engages computers to learn from data and excels at identifying complex patterns within large datasets, enabling predictive models that can personalise treatment.
Selecting the optimal ML approach for a given clinical task can introduce a fundamental trade-off: while more sophisticated algorithms (e.g. deep learning) can model complex biological systems with greater accuracy, they often sacrifice transparency in their decision-making rationale. In clinical settings, this lack of interpretability poses a critical challenge, as clinicians prefer to understand the reasoning behind AI-generated recommendations to maintain trust. That said, our inability to understand AI-driven recommendations does not necessarily mean that they are incorrect, and such a stipulation could stifle advancement. It could be argued that we often use technologies in modern life that we do not fully understand.
Nevertheless, at least in the short term, clinical supervision is required to avoid implementation of decisions that would not be in keeping with defensible clinical practice, especially as clinical responsibility still lies with the treating clinician. Consequently, AI is unlikely to replace clinical expertise but rather to augment it with intelligent tools to reach better, faster decisions.
TRANSFORMING AN ART INTO A SCIENCE
Whilst IVF protocols are designed to work for most people, with the typical patient in mind, clinicians use their experience and skill to adapt protocols and personalise treatment, although this can be subjective and inconsistent. Thus, it is often said that assisted reproductive technology (ART) is as much an art as science, with clinicians often donning their whites to ‘cook’ up a new recipe. Additionally, IVF cycles produce a large amount of complex data that are hard to fully assimilate when clinicians make treatment decisions, leading to ‘rules of thumb’ to simplify the data so that it is comprehensible.
An example of this simplification is the monitoring of folliculogenesis during ovarian stimulation. Here, supraphysiological doses of follicle-stimulating hormone (FSH) are used to stimulate growth of multiple follicles, so that they can undergo oocyte maturation in response to luteinising hormone (LH)-like exposure (called the trigger of oocyte maturation), in readiness for fertilisation. Follicles that are either too small or too large are less likely to respond to the trigger. However, the optimal size of follicles that can respond is not known.
In current practice, the largest follicle (or ‘lead’ follicle) is used to represent the entire cohort of growing follicles, and the trigger is given when two or three lead follicles reach 17–18mm in size, depending on the unit’s protocol. However, lead follicles may not reliably represent the sizes of the entire follicle cohort. So, while this simplification is practical, it does not optimise outcomes for an individual patient. AI is ideally suited to handling such complex data, enabling full use of the available information about each follicle in the entire follicle cohort.
'Many novel AI technologies are offered to clinics commercially with an associated cost, and the ‘inconvenient reality’ is that many have not been validated in a scientifically robust manner.'
To address this complexity, our multidisciplinary research team at Imperial College London, comprising both healthcare professionals and AI specialists, used explainable AI methods to identify the specific follicle sizes most likely to yield mature oocytes. Leveraging data from over 19,000 patients, we found that maximising the proportion of follicles within the optimal follicle size range not only improved mature oocyte yield but, importantly, also the chance of live birth.2 Additionally, we noted that continuing ovarian stimulation for too long resulted in follicles larger than the identified optimal size that secrete progesterone, prematurely advancing the endometrium such that it is out of sync with embryo development, to the detriment of pregnancy rates. These AI-derived insights can help personalise IVF treatment decisions and optimise clinical outcomes for each patient.
MANAGING THE TRANSITION TO CLINICAL PRACTICE
Robust prospective validation remains a cornerstone prior to implementation to clinical practice. New reporting guidelines, such as TRIPOD+AI, help address this challenge by mandating transparent reporting and independent assessment of AI systems. Achieving the perfect balance between cutting-edge innovation, regulatory approval and adequate validation is no simple feat.
One of the few trials that aimed to demonstrate non-inferiority of an AI-assisted embryo selection with time-lapse incubation perfectly illustrated this challenge.3 While the AI system significantly reduced evaluation time compared with manual assessment by an embryologist, live birth rates remained statistically inferior. Trials are time-consuming to set up and to conduct, which is not ideal when assessing the validity of such fast-moving technologies, where the algorithm tested could be outdated by the time a trial can be conducted. However, this trial highlights that the supposition of improved efficacy and avoidance of harm with a novel AI method trained on retrospective data should not be assumed without prospective validation. Indeed, many novel AI technologies are offered to clinics commercially with an associated cost, and the ‘inconvenient reality’ is that many have not been validated in a scientifically robust manner.4
IN SUMMARY
The potential for AI to optimise IVF treatment is vast, but its success depends on our willingness to embrace evidence-based innovation while maintaining the highest standards of rigour in scientific evaluation.
The path forward requires collaboration between clinicians, scientists, AI engineers, industry and regulators. Efficient methods for prospective evaluation of such fast-moving technologies are a significant challenge to ensure efficient and continuous evaluation of non-static technologies. Nevertheless, AI has huge potential to transform fertility treatment and optimise care for those suffering from infertility, in an objective, data-driven manner.
SIMON HANASSAB
PhD Researcher in Healthcare AI, Imperial College London
ALI ABBARA
Associate Professor in Endocrinology, Imperial College London
REFERENCES
1. Hanassab S et al. 2024 npj Digital Medicine https://doi.org/10.1038/s41746-024-01006-x.
2. Hanassab S et al. 2025 Nature Communications https://doi.org/10.1038/s41467-024-55301-y.
3. Illingworth PJ et al. 2024 Nature Medicine https://doi.org/10.1038/s41591-024-03166-5.
4. Kieslinger DC et al. 2024 Nature Medicine https://doi.org/10.1038/s41591-024-03289-9.

{kind=link}