Despite significant investment in genomics and genetics, observations across the illness spectrum – from apparently super-healthy individuals to those with severe disease – have only rarely resulted in new drugs for patients. In metabolic disease, however, there has been at least limited success; the discoveries of insulin, glucagon-like peptide-1 (GLP-1) agonists and sodium–glucose cotransporter-2 (SGLT2) inhibitors all resulted from near-chance observations in dogs and humans.
Banting and Best isolated ‘isletin’ from pancreatic extracts of dogs and then cattle, to finally demonstrate in patients that insulin was able to keep diabetic patients alive.1 Observations on the incretin effect and the eating patterns of the Gila monster resulted in the discovery of stable GLP-1 agonists (marketed as exenatide) and from there, based on the human GLP-1 sequence, stabilised variants of the human GLP-1 peptide. Finally, identification of naturally occurring mutations in the SGLT2 transporter, coupled with the effect of phlorizin, led to the discovery of the growing class of SGLT2 inhibitors. Because both the GLP-1 and the SGLT2 inhibitor classes have shown long term cardiovascular, renal and heart failure benefits, all three discoveries may also have in common a likelihood that they will form the basis of modern diabetes treatment in the 21st century.
Although these and other blood glucose-lowering agents have helped us gain some ground in the battle for control of type 2 diabetes, all offer only a delay of disease progression (‘treat to fail’), as medication regimens gradually increase while β-cells progressively fail to meet insulin demand and body weight steadily rises. This continues to drive the search for agents that can deliver a step change in weight loss and provide glycaemic control that is as effective as insulin. Such an agent might be able to treat, to cure or at least halt disease progression.
WHERE NEXT FOR DIABETES RESEARCH?

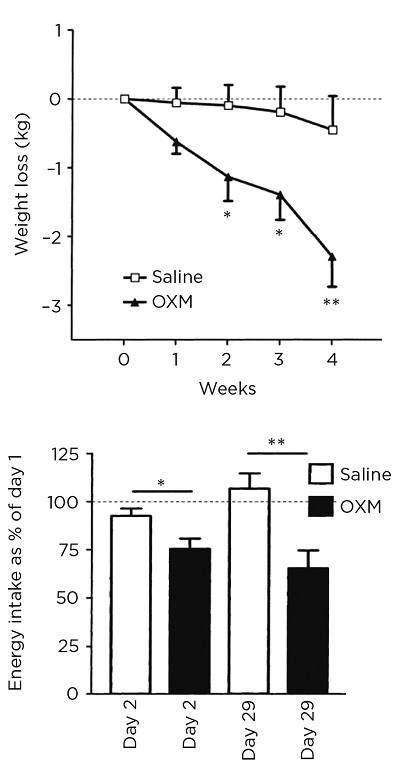
Figure 1. Initial observations by Wynne et al. (2) on the metabolic effects of oxyntomodulin (OXM). *P<0.05; **P<0.005. Republished with permission of American Diabetes Association, from 'Subcutaneous oxyntomodulin reduces body weight in overweight and obese subjects: a double-blind, randomized, controlled trial'; Diabetes 2005 54 2390-2395; permission conveyed through Copyright Clearance Center, Inc.
A possible next step forward in diabetes research might come from work conducted on a still rather less well-known peptide hormone by Steve Bloom’s group at Imperial College London in the late 1990s.2 They researched the effects of oxyntomodulin, a naturally occurring 37-amino acid peptide, levels of which are increased in patients who have undergone bariatric surgery.
Oxyntomodulin, which is derived from the same gene as GLP-1 but is the result of differential proteolytic cleavage of the pro-peptide, is a dual agonist with both glucagon and GLP-1 activity, with a strong bias toward glucagon. In a 4-week clinical study published in 2005, healthy overweight and obese volunteers were injected with oxyntomodulin 30 minutes before each meal. A weight reduction of 2.3kg was seen, versus a weight reduction of 0.5kg in the comparator group (Figure 1). The larger weight reduction was associated with a reduction in energy intake of 250kcal at the final test meal.2
A further study by the same group showed an increase in activity-related energy expenditure, total energy expenditure and overall physical activity.3 Despite these findings, scepticism about the data persisted because the strong glucagon tone of oxyntomodulin was seen as a significant concern when considering these data for an anti-diabetic therapeutic approach.
MEDIMMUNE ENTERS THE PICTURE
The physical and chemical properties of oxyntomodulin make it a suboptimal choice for an effective drug. It has a half-life in the circulation of less than 12 minutes, is cleaved readily by serum proteases and is very hydrophobic and therefore difficult to formulate. Engineering its stability might have been an easy task, but changing the peptide’s serum half-life might require changes to the balance of glucagon and GLP-1 activity to preserve its overall efficacy.
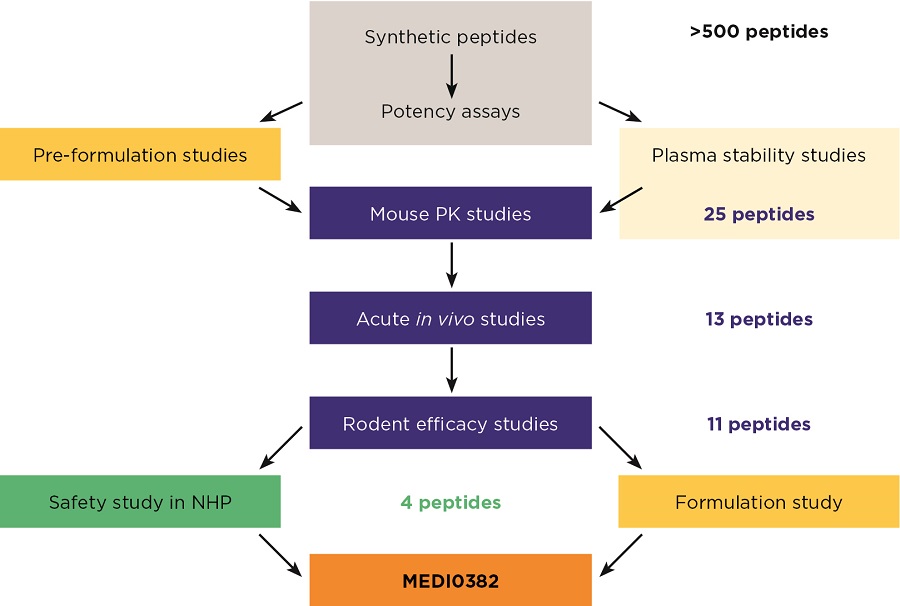
These peptides were then rigorously tested (Figure 2). Initially, their potency was assessed in vitro by incubating them with Chinese hamster ovary cell lines that expressed rodent or human GLP-1 and glucagon receptors. In addition, ex vivo studies using primary rodent hepatocytes assessed glucose output to gauge the level of glucagon-like activity and evaluated insulin secretion to gauge the level of GLP-1-like activity.
Natural peptides tend to aggregate and form amyloids when incubated at high concentrations for prolonged periods, because their natural function is to be active at low concentrations and to circulate in the blood for only a few minutes. All peptides were therefore assessed in parallel for their ‘manufacturability’ and their ability to be formulated and stored at high concentrations.
Preliminary lead peptides were then further characterised in animal models, which are crucial to building confidence in a potential peptide therapy. Studies conducted for the MedImmune lead peptide, MEDI0382, included both acute and chronic administration in rodent disease models and chronic dosing in healthy cynomolgus monkeys to assess safety before being tested for the first time in humans. Many years of work on more than 500 peptide candidates culminated in the selection of MEDI0382 for progression into the clinic,4 but this is only the next phase of a long journey to become a marketed product.

Figure 2. Discovery of MEDI0382, an oxyntomodulin-like peptide for treatment of type 2 diabetes and obesity (2). NHP=non-human primate; PK=pharmacokinetics
INTO THE CLINIC
Data on dose ranges of drugs in humans come initially from a single ascending dose (SAD) study. Originally conducted only in healthy volunteers, SAD studies are increasingly conducted in the target population for the drug. In this case, however, because MEDI0382 represents a potential member of a new class of medications for diabetes, studies were conducted in healthy volunteers.
The SAD study is followed by the multiple ascending dose (MAD) study, in which the effect of the drug is properly evaluated in the target population, in this case patients with type 2 diabetes. MAD studies typically involve treating between 40 and 60 patients with the disease. The studies last for a few weeks and are designed to inform the design of the phase 2b and phase 3 study programmes.
With respect to diabetes, the SAD and MAD studies represent the end of the beginning, not the beginning of the end, of the testing programme. To gain a diabetes indication, the potential drug will be tested in an additional 4,500 patients on average in phase 2b and 3 trials, coupled with a cardiovascular outcome study of 6,000 to 9,000 patients. Only when these studies are successfully completed can a drug make it to, and stay on, the market.
CONCLUSION
It’s a labour of love to take an observation from the clinic to make a medicine for patients, which requires years of time and millions of pounds to achieve success. Nevertheless, unmet targets for metabolic and endocrine disease remain, and as a medical community it is imperative that we strive to meet them. Pharmaceutical companies are always interested in hearing about potential new targets for therapeutic intervention, and MedImmune is no exception.
Phil Ambery & Lutz Jermutus
MedImmune Ltd, Granta Park, Cambridge
REFERENCES
1. Banting FG et al. 1922 Canadian Medical Association Journal 12 141–146.
2. Wynne K et al. 2005 Diabetes 54 2390–2395.
3. Wynne K et al. 2006 International Journal of Obesity (London) 30 1729–1736.
4. Henderson SJ et al. 2016 Diabetes Obesity & Metabolism 18 1176–1190.




{kind=link}
{kind=link}