Our understanding of the significance of sex hormones as drivers of endocrine-related cancer originates from key historical studies by Beatson (oophorectomy) and Huggins (adrenalectomy) in the treatment of patients with advanced disease.1,2 Since the late 20th century, there have been tremendous pharmacological advances in targeting the endocrine drivers of the two most common endocrine-related cancers: breast and prostate cancer. Today, patients can expect much more favourable outcomes.
However, resistance to endocrine therapies is inevitable, with approximately 30% of endocrine-treated breast cancer patients experiencing disease progression. Consequently, uncertainties remain regarding the precise steroid drivers of the disease.3,4 There is, therefore, still much to be understood in the areas of tumour intracrinology, the influence of body composition on steroid production, and cellular responses to complex mixtures of steroid hormones. Of particular relevance in breast cancer research are the poorly understood consequences of menopause hormone therapy use, both by survivors of breast cancer and by individuals at increased risk of developing the disease.5
A NEW TOOL FOR INVESTIGATING ENDOCRINE-RESISTANT DISEASE

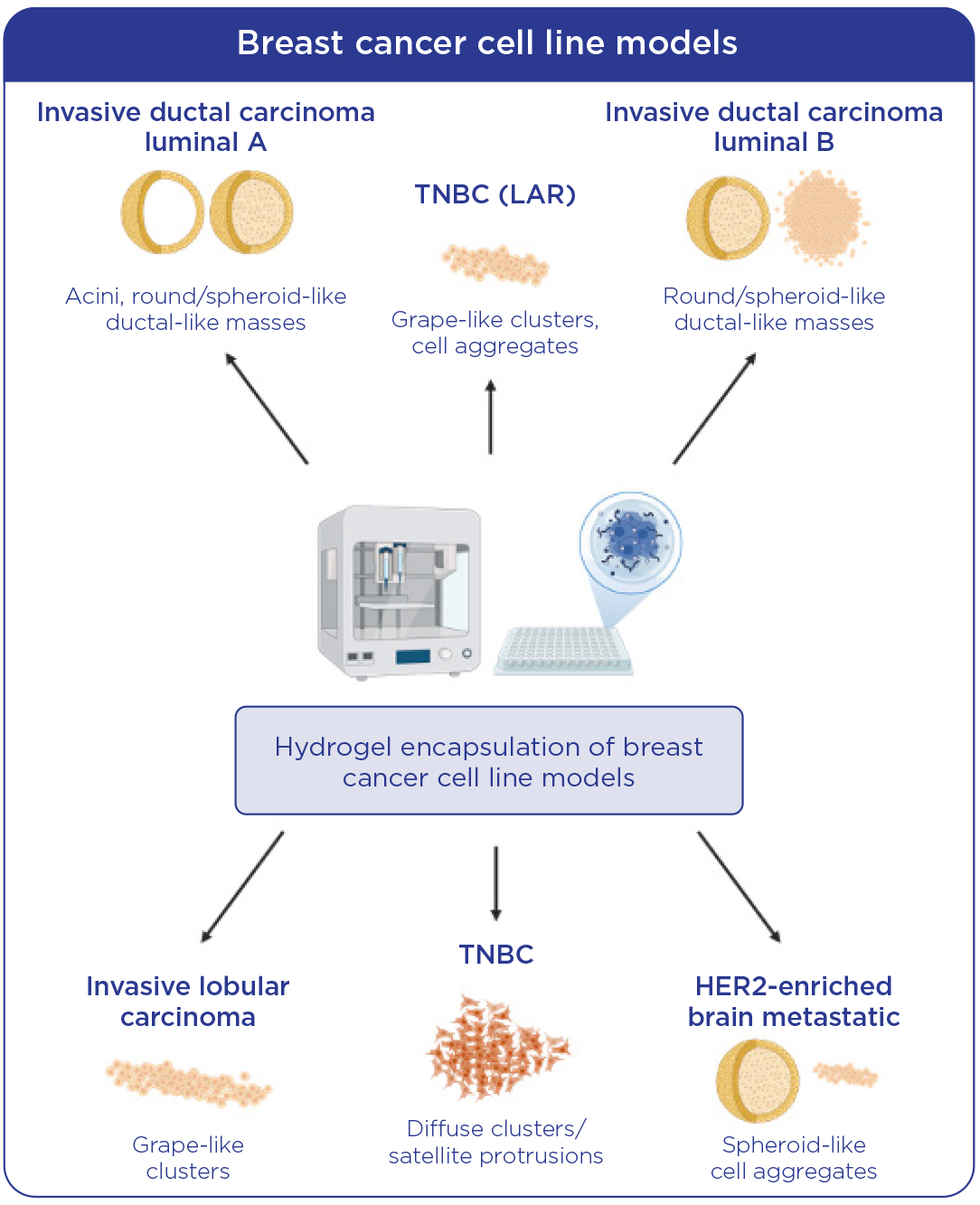
Schema illustrating the various structures formed by breast cancer cell line subtypes when bioprinted in 3D hydrogel. LAR, luminal androgen receptor-positive; TNBC, triple-negative breast cancer. Created with BioRender
Breast cancer research has traditionally been conducted using a wide range of patient-derived cell lines, reflecting various subtypes. Over the past decade, there has been a rapid expansion in the development of patient-derived xenograft and organoid models of disease. These sophisticated models provide the opportunity to evaluate the tumorigenic potential and tumour cell interactions within the in vivo microenvironment. However, the low tumour take-rate and the long duration (>18 months) required for tumours to grow to a sufficient volume are major limitations of these models, especially for hormone receptor-positive breast cancers.
Our group has been exploring the utility of a synthetic, xeno-free hydrogel 3D bioprinting approach to provide a more robust, time-efficient model system for the 3D propagation of breast cancer cell lines and primary breast tumours. Modern drop-on-demand bioprinting systems offer a highly reliable, sterile and reproducible platform for generating 3D tumour structures that accurately recreate the growth patterns of breast cancer subtypes within a matrix that mimics the stiffness of normal breast tissue. This approach enables the modelling of cell–cell interactions, cell–extracellular matrix interactions, and potentially, cell–drug interactions.
Using this platform, we have developed a comprehensive panel of 3D bioprinted breast cancer cell line subtypes, including luminal A and B, lobular, luminal androgen receptor-positive, triple-negative breast cancer and brain metastatic subtypes (see Figure). The structures formed have been characterised to reflect not only hormone receptor status (oestrogen receptor-α, progesterone receptor, androgen receptor) but also the degree of inter-epithelial and epithelial–extracellular matrix interaction (ZO-1, epithelial cell adhesion molecule, F-actin). In our hands, 3D bioprinting of primary tumours closely mirrors the breast cancer subtype (invasive ductal carcinoma or lobular), matching the gold-standard mammary intraductal model.6
SEX STEROIDOGENESIS: A UNIQUELY HUMAN CONDITION
Human endocrinology is unique even among mammals, with only humans and certain species of whale undergoing menopausal transition. Importantly, after menopause, a considerable proportion of steroid hormones are of adrenal origin, in stark contrast to rodents, whose sex hormones are all gonadally driven. Thus, in vivo models involving oophorectomy and steroid supplementation do not accurately recapitulate the aged, postmenopausal breast cancer environment.
‘Establishing humanised endocrine models of breast cancer will enhance our understanding of both genomic and nongenomic sex steroid actions.’
With this in mind, we have specifically utilised 3D bioprinted models of breast cancer to explore the often-neglected endocrine environment, which is crucial to understanding resistance to oestrogen/oestrogen receptor-targeting therapies. We and others have highlighted the tumour-potentiating role of the postmenopausal androgenic steroid milieu, particularly in the setting of aromatase inhibitor resistance. Androgen excess is well established as perturbing metabolism in women, and renewed interest in adrenal-derived subclasses, such as the 11-oxygenated androgens, as drivers of pathology makes them of particular interest in postmenopausal breast cancers, which significantly associate with metabolic syndrome and obesity.7
While we have extensive clinical data highlighting the link between androgens as drivers of disordered metabolism, our understanding of the exact mechanisms remains incomplete. Understanding how the patient’s steroid hormone profile impacts tumour behaviour is often neglected. Moreover, typical analysis of steroid hormone impact is often limited to the most potent, yet least abundant, steroids, and focuses on genomic action within the tumour cell.
Studies on the impact of androgen excess on health and disease in women suggest that more abundant, lower affinity ligands are often more significantly associated with the disease state.8,9
To address this, we have utilised conditioned medium from primary tumour-associated adipocytes exposed to pro-hormone androstenedione, and subsequently profiled by liquid chromatography tandem mass spectrometry, to evaluate the impact in 3D bioprinted models of disease. The development of more complex endocrine models of resistant breast cancer utilising this platform may help elucidate the interplay amongst the cognate steroid receptors when exposed to physiologically relevant levels of hormones arising in the mammary microenvironment.
CONCLUSION
Establishing humanised endocrine models of breast cancer will enhance our understanding of both genomic and non-genomic sex steroid actions. With the recent 2025 Food and Drug Administration guidelines ushering in a new era of drug discovery, which does not rely on expensive and often ineffective in vivo studies, integrating these more physiologically relevant endocrine models could become a reliable and cost-effective new approach methodology in drug development.10
STEPHANIE AGBANA
PhD Student, Department of Surgery, Androgens in Health and Disease Research Group; and RCSI University of Medicine and Health Sciences, Dublin, Ireland
MICHAEL O’REILLY
Consultant Endocrinologist, Department of Endocrinology, Androgens in Health and Disease Research Group; RCSI University of Medicine and Health Sciences; and Beaumont Hospital, Dublin, Ireland
MARIE McILROY
Senior Lecturer, Department of Surgery, Androgens in Health and Disease Research Group; and RCSI University of Medicine and Health Sciences, Dublin, Ireland
REFERENCES
1. Beatson GT 1896 Transactions Medical Chirurgical Society of Edinburgh https://pmc.ncbi.nlm.nih.gov/articles/PMC5518378.
2. Huggins C & Bergenstal DM 1952 Cancer Research 12 134–141.
3. Morgentaler A 2008 Journal of Sexual Medicine https://doi.org/10.1111/j.1743-6109.2008.00889.x.
4. Jordan VC 2008 Journal of Clinical Oncology https://doi.org/10.1200/JCO.2008.17.5190.
5. Chuffa LG et al. 2017 Steroids https://doi.org/10.1016/j.steroids.2016.12.011.
6. Kittrell F et al. 2016 Bio-Protocol https://doi.org/10.21769/bioprotoc.1744.
7. Buono G et al. 2020 Breast Cancer Research & Treatment https://doi.org/10.1007/s10549-020-05701-7.
8. O’Reilly MW et al. 2014 Journal of Clinical Endocrinology & Metabolism https://doi.org/10.1210/jc.2013-3399.
9. Bleach R et al. 2021 Clinical Cancer Research https://doi.org/10.1158/1078-0432.CCR-20-4135.
10. Food & Drug Administration 2025 Roadmap to Reducing Animal Testing in Preclinical Safety Studies https://www.fda.gov/media/186092/download.

{kind=link}