Prior to 2010, hypophysitis was a rare condition, mostly seen in the post partum period or due to IgG4-related disease. However, that changed with the introduction of ipilimumab, a cytotoxic T-lymphocyte antigen-4 (CTLA-4) inhibitor, also termed an immune checkpoint inhibitor, which was among the first treatments to show survival benefit in melanoma.
SIDE EFFECTS OF CHECKPOINT INHIBITORS

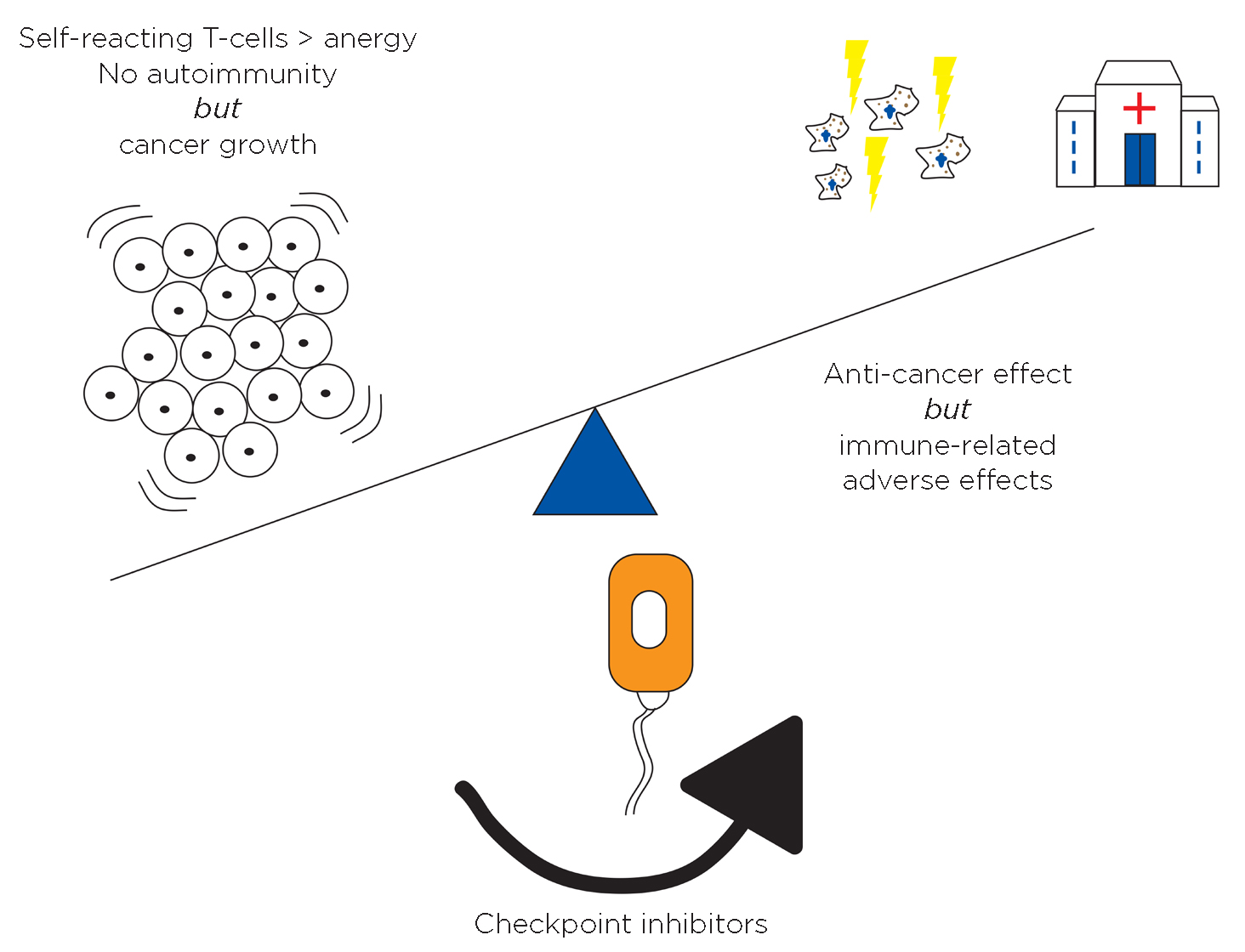
The relationship between anti-cancer effects of checkpoint inhibitors and immune- related events, including endocrine dysfunction. Reproduced from Anderson & Morganstein8 under CC BY-NC 4.0 licence. ©The Authors 2021.
It rapidly became apparent that ipilimumab also caused a presumed immune-mediated hypophysitis in up to 10% of patients. This frequently presents with headache, occasionally with pituitary enlargement significant enough to impact the optic chiasm, and with near-universal hypopituitarism.1 It is now well recognised that pituitary dysfunction can also frequently occur without clear-cut evidence of pituitary inflammation.
Checkpoint inhibitors target naturally occurring immune checkpoints – co-regulators of T-cell function that drive self-reacting T-cells to anergy, for example CTLA-4 interacting with B7-1 expressed on antigen-presenting cells. Blocking this leads to enhanced T-cell activation against the cancer cells, but also to a risk of immune-related adverse events (see Figure).
Subsequent developments led to drugs blocking the interaction between programmed cell death-1 (PD-1) and programmed cell death ligand-1 (PD-L1) on more mature T-cells. This pathway is exploited by many cancer cells that over-express PD-L1 to avoid immune detection.2 Drugs targeting this PD-1/PD-L1 interaction are now widely used in many different cancers, including in adjuvant treatment, or increasingly (as in breast cancer) in the neo-adjuvant setting prior to surgery.
PD-1/PD-L1 inhibitors show a different pattern of pituitary dysfunction, with actual hypophysitis being rare, but isolated adrenocorticotrophin (ACTH) deficiency developing in up to 2% of treated individuals.3 However, as these drugs are now much more widely used than ipilimumab, this is translating to ever-increasing numbers of affected patients. Transient secondary hypothyroidism and hypogonadism are described less commonly than with ipilimumab, and may recover with both drugs. The striking finding, however, is that ACTH deficiency is permanent, leading to a life-long need for glucocorticoid replacement.4
RECOGNISING THEIR ENDOCRINE IMPACT
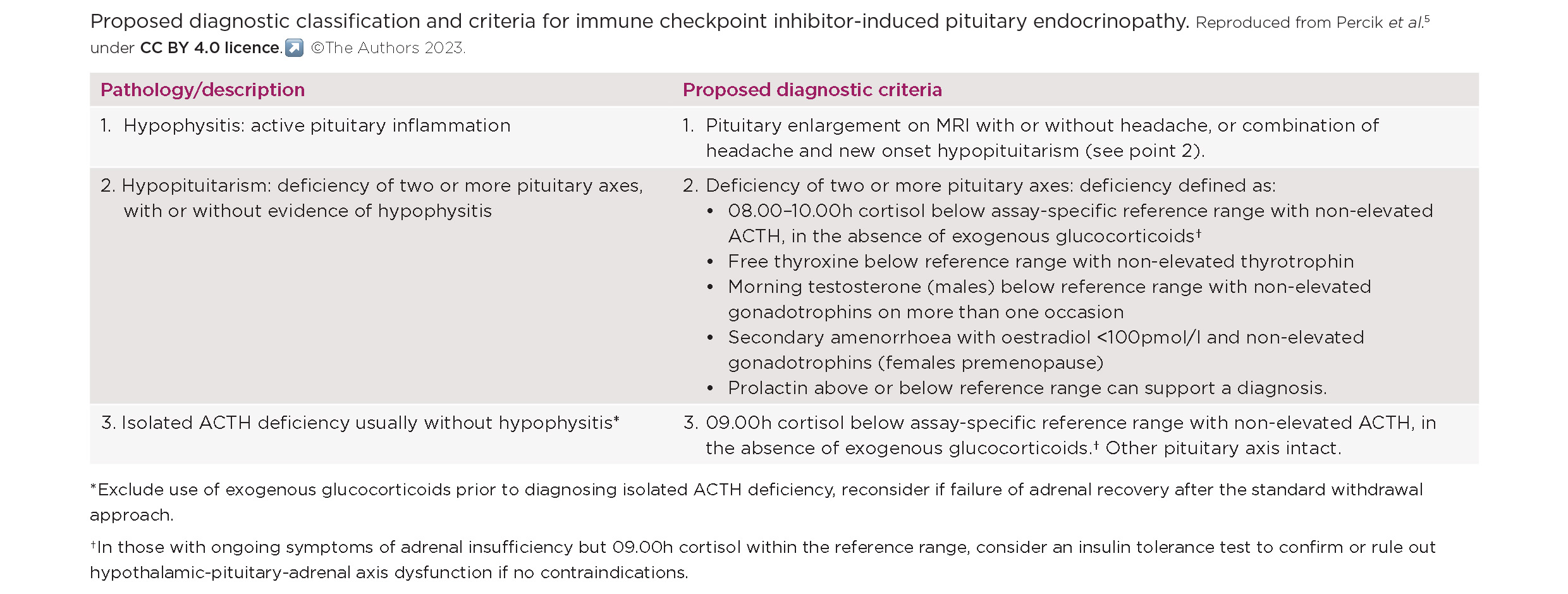
The oncology literature frequently reports all pituitary abnormalities as hypophysitis, which can make it challenging to truly understand the impact of checkpoint inhibitors on the pituitary. In fact, from the viewpoint of an endocrinologist, there are three distinct presentations: hypophysitis (which usually, but not always, leads to hypopituitarism), hypopituitarism and isolated ACTH deficiency. A recent position statement, endorsed by the Society for Endocrinology, has suggested an endocrine classification on this basis (see Table). Using this classification will ensure correct endocrine management.5
A key practice point, therefore, is that whilst some people will present with symptoms of an actual hypophysitis, with headache, pituitary dysfunction and an enlarged pituitary on magnetic resonance imaging, many more will only have symptoms of adrenal insufficiency due to isolated ACTH deficiency.
Recognition is made more challenging by two points. The first is that symptoms of adrenal insufficiency, especially fatigue, are common in people with advanced cancer even in the absence of endocrine dysfunction, so a high degree of clinical suspicion is needed to ensure prompt measurement of morning cortisol when there are even subtle changes in symptoms.
The second is that steroids are frequently used in oncological practice. A third of patients treated with a checkpoint inhibitor will need high-dose steroids to treat non-endocrine adverse events.6 Checkpoint inhibitors are increasingly used in combination with conventional chemotherapy, where dexamethasone is frequently used as an anti-emetic. Thus, careful assessment is required when assessing cortisol levels to ensure correct diagnosis of ACTH deficiency as opposed to adrenal suppression. This is especially important when the checkpoint inhibitor is used as part of a neo-adjuvant treatment approach, to ensure that adrenal insufficiency is not missed prior to elective surgery.
CLINICAL MANAGEMENT
'...prompt assessment of cortisol levels at the onset of symptoms remains vital to ensure those developing ACTH deficiency are treated with glucocorticoid replacement before the onset of adrenal crisis'
All guidelines and the Summary of Product Characteristics for checkpoint inhibitors recommend monitoring for changes in thyroid function before and during treatment. This leads to the question of whether there is clinical utility in monitoring cortisol levels during treatment to allow earlier detection of ACTH deficiency. One study suggested that, when it was practical to monitor early morning cortisol levels, it was possible to diagnose ACTH deficiency earlier. When detected it can safely be managed as an outpatient with prompt glucocorticoid replacement. However, more recent data show that the onset of adrenal insufficiency is rapid, with a gap from the last normal cortisol to the onset of adrenal insufficiency sometimes as short as a few days.7
This suggests that screening is unlikely to be practical, and prompt assessment of cortisol levels at the onset of symptoms remains vital to ensure those developing ACTH deficiency are treated with glucocorticoid replacement before the onset of adrenal crisis, wherever possible. This can be particularly challenging when morning cortisol levels are indeterminate, as synacthen tests will not be reliable, given the rapid onset of ACTH deficiency, and many patients with cancer will not be able to have insulin tolerance tests. Therefore, in this situation, repeat testing after a few days may be most appropriate, covering with glucocorticoid replacement if unwell (for example with a fever). It remains unclear whether partial ACTH deficiency can occur and, in the case of persistent indeterminate cortisol levels, individual clinical assessment is required.
In conclusion, whilst immunotherapy with checkpoint inhibitors represents a major advance in cancer treatment, it is also posing new challenges to endocrinologists who need to be ready to diagnose and follow up this rapidly increasing cohort of patients with life-long iatrogenic endocrine dysfunction.
DANIEL L MORGANSTEIN
Department of Endocrinology, Chelsea and Westminster Hospital, and Royal Marsden Hospital, London
REFERENCES
1. Faje A 2016 Pituitary https://doi.org/10.1007/s11102-015-0671-4.
2. Pardoll DM 2012 Nature Reviews Cancer https://doi.org/10.1038/nrc3239.
3. Percik R et al. 2020 Autoimmunity Reviews https://doi.org/10.1016/j.autrev.2019.102454.
4. Faje A et al. 2019 European Journal of Endocrinology https://doi.org/10.1530/eje-19-0238.
5. Percik R et al. 2023 Endocrine Connections https://doi.org/10.1530/EC-22-0513.
6. Agarwal K et al. 2020 Clinical Medicine https://doi.org/10.7861/clinmed.2018-0440.
7. Seejore K et al. 2022 European Journal of Endocrinology https://doi.org/10.1530/eje-21-0760.
8. Anderson B & Morganstein DL 2021 Endocrine Connections https://doi.org/10.1530/EC-20-0489.


{kind=link}
{kind=link}