Why do we need vitamin D?
Vitamin D deficiency is associated with disorders of bone and mineral metabolism and, in particular, the development of rickets and osteomalacia. However, there is growing evidence that vitamin D has a crucial role in the immune system: facilitating the normal response to infection and regulating inflammatory responses and autoimmune disease. It also maintains muscle strength, may prevent falls, and could lower the risk of developing cancer, cardiovascular disease and diabetes.
How do we obtain it?
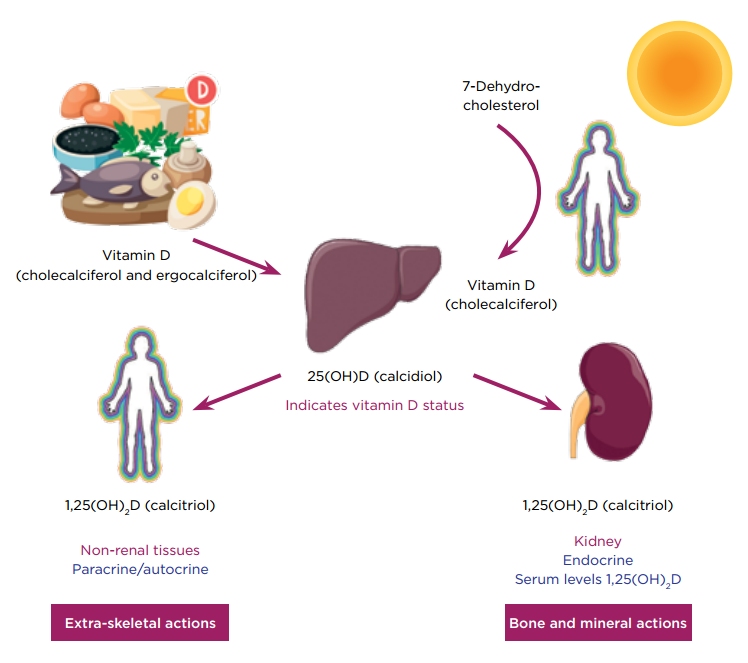
Vitamin D is found in foods such as oily fish, dairy products and mushrooms. However, for most people, the dietary intake of vitamin D is relatively low and the majority of it is synthesised (Figure). The key step is the conversion of 7-dehydrocholesterol in the skin to vitamin D (cholecalciferol), a reaction mediated by ultraviolet light (wavelength 290–320nm). Production of 25-hydroxyvitamin D (25(OH)D; calcidiol) by the liver is dependent on vitamin D availability. As such, serum 25(OH)D is considered a good indicator of vitamin D status.

Vitamin D is obtained from the diet or synthesised in the skin by the conversion of 7-dehydrocholesterol, a reaction mediated by UV light (290–320nm). Hydroxylation of vitamin D in the liver produces 25-hydroxyvitamin D (25(OH)D; calcidiol). A further hydroxylation step, catalysed by 25(OH)D 1α-hydroxylase, produces the active hormone 1,25-dihydroxyvitamin D (1,25(OH)2D; calcitriol). Liver/kidneys ©Servier Medical Art; Person ©Clipart.co; Vitamin D ©Shutterstock
How much do we need?
There isn’t a consensus on what constitutes a healthy vitamin D level. Vitamin D isn’t considered in terms of a normal range. Instead, people are classified as having deficient, insufficient or adequate levels of serum 25(OH)D. But where should those boundaries lie? Are the serum 25(OH)D thresholds required to maintain skeletal health the same as those required for extra-skeletal outcomes, and do thresholds vary with population subgroups?
The National Osteoporosis Society suggests that a level <30nmol/l is deficient, 30–50nmol/l is insufficient and >50nmol/l is adequate.1 The Scientific Advisory Committee on Nutrition (SACN) is currently reviewing guidance for vitamin D. The draft report was published in 2015 with the final report due later this year. They concluded that, to ensure the musculoskeletal health of the population (97.5% of individuals) is protected, serum 25(OH)D levels should not fall below 25nmol/l at any time of the year.2
Although most people in the field were disappointed that they had set the level so low (the Institute of Medicine concluded that serum 25(OH)D levels should be 50nmol/l), we should remember that this is an absolute minimum for everyone.
How widespread is the deficiency?
Data from the National Diet and Nutrition Survey indicated that, across the year, 21.8% of all UK adults were deficient (<25nmol/l) and 61.4% had insufficient levels (><50nmol/l). These percentages increased significantly in certain populations, with 53–80% of adult Asian women having serum 25(OH)D below 25nmol/l. This is reflected across Europe, although notable exceptions were found, such as in Greece!3 Deficiency in young children is significant, and is manifested by an increase in rickets.
How can we maintain adequate levels?
Sunlight exposure correlates with 25(OH)D levels. Until very recently, it had been thought that advocating safe sun exposure (10–15 minutes per day in the summer) coupled with a healthy diet would ensure adequate vitamin D levels (currently supplements are only recommended for individuals at risk of deficiency). However, this is unlikely to be the case.
This is where the SACN recommendations make interesting, although possibly controversial, reading. SACN calculated that, to achieve a serum 25(OH)D ≥25nmol/l in winter, it is necessary to have a vitamin D intake of approximately 10µg (400IU) per day. It is unlikely that this could be achieved by a change in diet. This leaves two options: food fortification or supplementation. Both options are controversial. Is it reasonable, or possible, to consider supplementing the whole population? Licensed vitamin D products have only been available in the UK for the last few years, and could everyone have a prescription for vitamin D? Over the counter >OH)D levels. Until very recently, it had been thought that advocating safe sun exposure (10–15 minutes per day in the summer) coupled with a healthy diet would ensure adequate vitamin D levels (currently supplements are only recommended for individuals at risk of deficiency). However, this is unlikely to be the case.
This is where the SACN recommendations make interesting, although possibly controversial, reading. SACN calculated that, to achieve a serum 25(OH)D ≥25nmol/l in winter, it is necessary to have a vitamin D intake of approximately 10µg (400IU) per day. It is unlikely that this could be achieved by a change in diet. This leaves two options: food fortification or supplementation.
Both options are controversial. Is it reasonable, or possible, to consider supplementing the whole population? Licensed vitamin D products have only been available in the UK for the last few years, and could everyone have a prescription for vitamin D? Over the counter vitamin D supplements are classified as health foods and are therefore not subject to the same controls as pharmaceutical products. The actual concentration of vitamin D per dose versus what is claimed by the products has been found to range from 14% to 150%, and they may contain potential allergens.
So what about food fortification? A few food items are voluntarily supplemented with vitamin D, and this is used positively in marketing material. However, the UK is generally reticent to accept mandatory food fortification, fluoride in water being the exception. Interestingly, there is an example of a widespread hormonal deficiency that was corrected by food fortification – that of iodine supplementation of salt to correct a worldwide thyroid hormone deficiency.
Awareness of vitamin D deficiency is growing; however there is a reluctance to accept the potential scale of the problem. It will be interesting to see the response to the SACN guidelines and how vitamin D deficiency is addressed in the next few years.
Rosemary Bland
University of Warwick and University Hospitals Coventry and Warwickshire NHS Trust
REFERENCES
- National Osteoporosis Society 2013 Vitamin D and Bone Health: A Practical Clinical Guideline for Patient Management http://bit.ly/26j74d3.
- Scientific Advisory Committee on Nutrition 2015 Draft Vitamin D and Health Report http://bit.ly/1NnG2uQ.
- Cashman KD et al. 2016 American Journal of Clinical Nutrition 103 1033–1044.


{kind=link}