A new year often brings new resolutions. Does ‘I’m going to exercise more this year’ sound familiar?
Often the main goal is to lose weight or more specifically, lose fat. (In this regard, Meerman and Brown provide an interesting insight into ‘When somebody loses weight, where does the fat go?’1) Based on the weight loss model of ‘calories in verses calories out’, undertaking regular exercise should help with this goal, although evidence shows that exercise alone may not be sufficient.2
Independent of weight loss, it is an incontrovertible truth that exercise is healthful. Any level of activity is associated with a 20% lower risk of mortality – even when it doesn’t reach the minimum national guidelines.3 So, what types of exercise should we be doing? At a basic level, we should undertake a combination of aerobic and strengthening activities.
AEROBIC ACTIVITY
Aerobic activity is often talked about in terms of intensity. The current NHS guidelines state ‘at least 150 min of moderate aerobic activity or 75 min of vigorous aerobic activity per week’. These have recently been updated to say ‘you can also achieve your weekly activity target with several short sessions of very vigorous intensity activity’. Moderate, vigorous, very vigorous – what do these mean? And does intensity really matter?
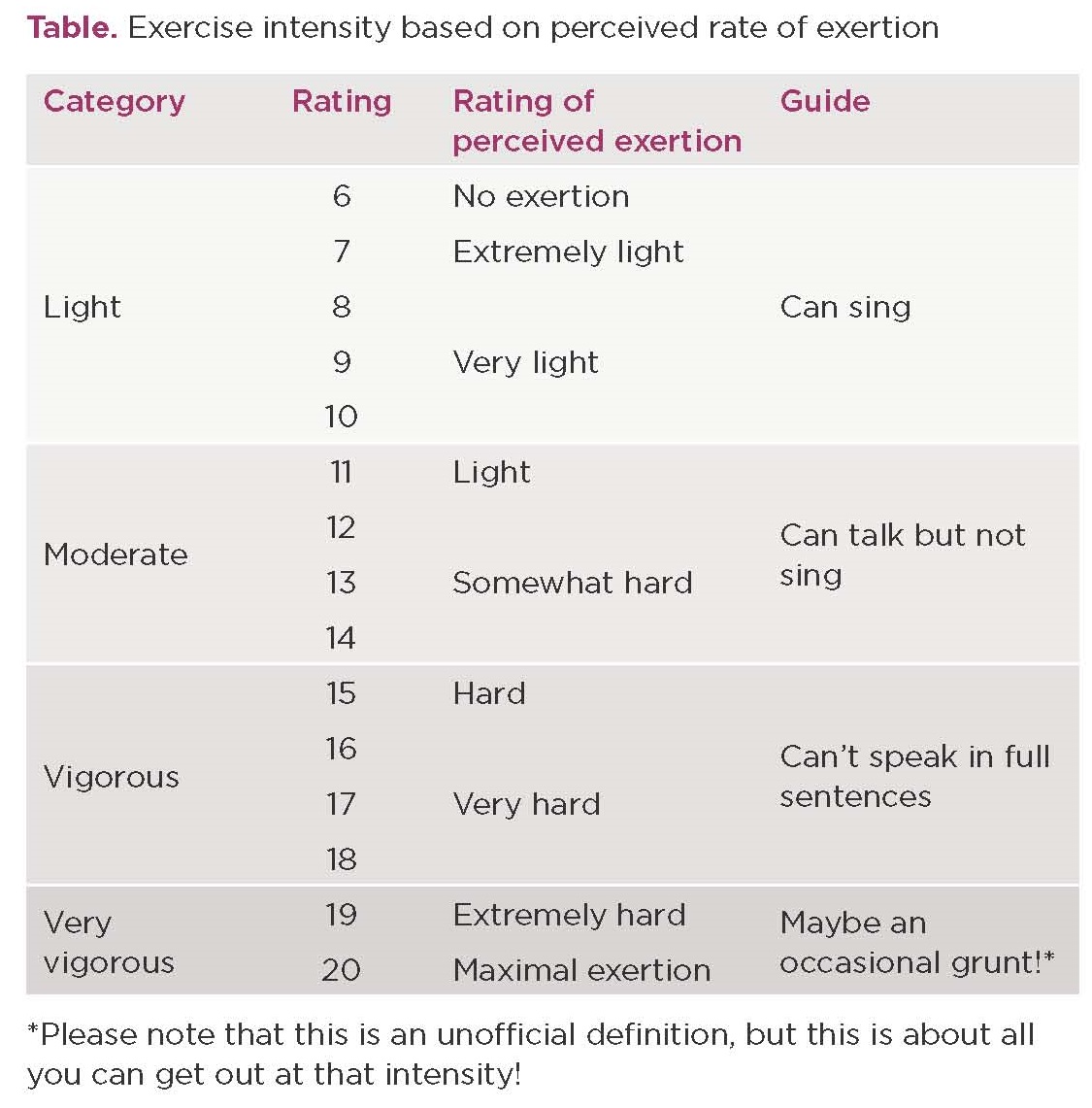
There are no universally accepted biochemical or physiological markers to distinguish between ‘light’, ‘moderate’, ‘vigorous’ and ‘very vigorous’ exercise intensities. Percentage of maximum heart rate is most commonly referred to; however, this is not always a reliable measure.4 Given its subjective nature, and the fact not everyone has or wears a heart rate monitor, then perhaps the best method to gauge exercise intensity is through perceived exertion (see Table).
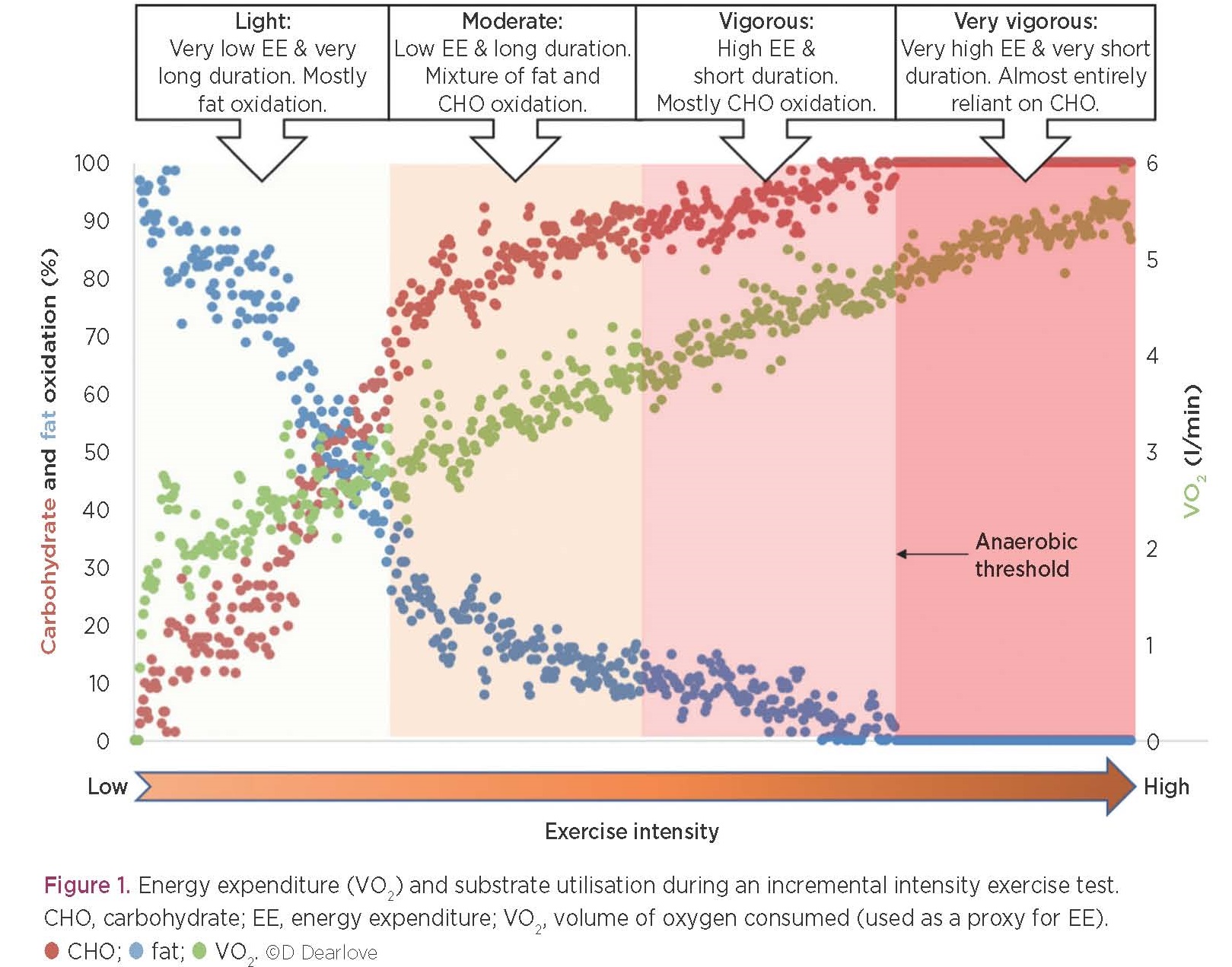
There is a linear relationship between energy expenditure (EE) and the intensity of exercise performed: the harder you work the more calories you burn (Figure 1). You’d have to exercise for approximately twice as long at a light–moderate intensity (~35% maximum) to burn the same number of calories as at a very vigorous intensity (~85% maximum).
THE UNDERLYING BIOCHEMISTRY
Given this, if your goal is weight loss, do you only need to exercise at a very vigorous intensity? Not necessarily, as at a very vigorous intensity your body is almost entirely reliant on carbohydrate (CHO) oxidation (mostly glucose derived from muscle glycogen) through mitochondrial and cytosolic glycolysis. Cytosolic glycolysis is a proton-producing pathway (contrary to widely held beliefs, these protons are not derived from the production of lactic acid5). Very approximately, the point at which you become entirely reliant upon glucose, with an increasing contribution to energy production from cytosolic glycolysis is referred to as the anaerobic threshold. Exercise above this threshold is painful and as such, cannot be sustained for extended periods. So, whilst you may be burning more calories, you cannot exercise for as long.
In contrast, if you exercise at moderate intensity (utilising a mixture of fat and CHO as substrates), you can keep going for longer and you need to ‘go for longer’ to burn the same number of calories. Indeed, longer duration, moderate intensity exercise and shorter duration, very vigorous exercise appear to be similarly efficacious for reducing body fat percentage.6
Regardless of the intensity, try to avoid consuming sports drinks whilst exercising. Even the leanest individual has enough fat to fuel low–moderate intensity activity for hours. Whilst CHO stores are more limited, unless you’re planning on exercising at a vigorous intensity for over an hour, sports drinks are still not necessary.
STRENGTHENING ACTIVITY
NHS guidelines also advocate muscle-strengthening activities such as lifting weights, typically called resistance training. Increasing and/or maintaining skeletal muscle mass is an important mediator of metabolic health, due to skeletal muscle’s prominent role in determining basal metabolic rate, mobility and stability.7
The regulation of skeletal muscle mass is determined by the balance between muscle protein synthesis (MPS) and muscle protein breakdown (MPB).8 Resistance exercise increases MPS for 24–48h, although net protein balance remains negative without protein/amino acid consumption.9 For the majority of individuals, sufficient protein can be consumed through dietary sources, rather than requiring specific supplements. Indeed, it has been reported that self-prescribed, spontaneous use of protein and CHO supplements by amateur men undertaking resistance training at gyms had no positive effects on body composition, compared with individuals who were not taking supplements.10
Guidelines regarding the optimal resistance training programmes to gain strength and build muscle are available.11,12 However, resistance exercise constitutes any action of skeletal muscle against external resistance, and therefore includes carrying heavy shopping bags or children, and activities such as digging in the garden. These latter options may be preferable introductions to resistance exercise for those who are less familiar/confident in the weights room.
WHAT ABOUT OTHER METABOLIC BENEFITS?
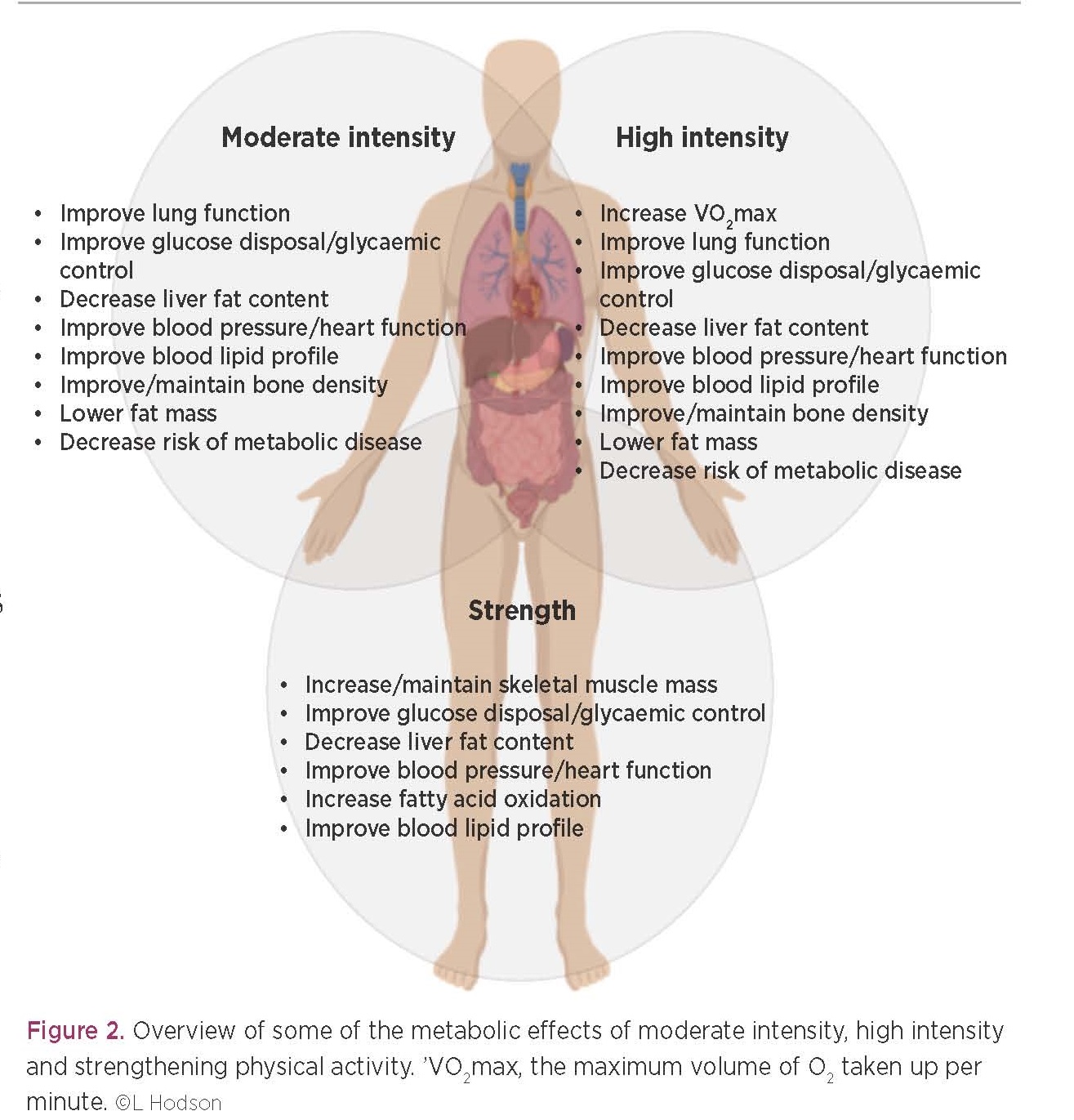
Undertaking a combination of aerobic and strengthening activities is encouraged, and there are many metabolic benefits to be gained from all forms of activity (Figure 2). For example, compared with moderate intensity exercise, vigorous to very vigorous exercise may increase VO2max (the maximum volume of O2 taken up per minute – an excellent indicator of metabolic health),13 result in greater or comparable improvements in insulin sensitivity and glycaemic control14 and cause larger decreases in systolic blood pressure.15 However, further work is required to determine whether a particular type/intensity of aerobic exercise is truly superior for long term health outcomes.
Strengthening activities aid in the regulation of glycaemic control and fatty acid oxidation. Indeed, an increased ratio of skeletal muscle to total body mass is inversely associated with cardiovascular disease risk, insulin resistance and type 2 diabetes.16,17 This becomes even more important with age, due to the gradual decline in muscle mass and strength that accompanies ageing (i.e. sarcopenia). This is associated with an increased risk of falls, disability and overall mortality.18
IN CONCLUSION
As the age-old saying goes, ‘every little helps’ – but to get the metabolic benefits of physical activity/exercise it needs to be undertaken regularly. Habit forming (and maintaining) is hard work but, as discussed, adding structured activity to you daily life has many health benefits.
Find what you enjoy and stick at it. If you are breathing a little harder or your muscles are straining, it’s almost certainly going to be having a beneficial effect.
David Dearlove, DPhil Candidate, Department of Physiology, Anatomy and Genetics, University of Oxford
Siôn Parry, Postdoctoral Research Assistant, Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford
Leanne Hodson, Professor of Metabolic Physiology, Oxford Centre for Diabetes, Endocrinology and Metabolism, University of Oxford
REFERENCES
- Meerman R & Brown AJ 2014 BMJ 349 g7257.
- Swift DL et al. 2018 Progress in Cardiovascular Disease 61 206–213.
- Arem H et al. 2015 JAMA Internal Medicine 175 959–967.
- Sarzynski MA et al. 2013 American Journal of Human Biology 25 695–701.
- Robergs RA et al. 2004 American Journal of Physiology – Regulatory, Integrative and Comparative Physiology 287 R502–R516.
- Viana RB et al. 2019 British Journal of Sports Medicine 53 655–664.
- Wolfe RR 2006 American Journal of Clinical Nutrition 84 475–482.
- Phillips BE et al. 2012 Current Opinion in Clinical Nutrition & Metabolic Care 15 58–63.
- Tipton KD & Wolfe RR 2001 International Journal of Sport Nutrition & Exercise Metabolism 11 109–132.
- Saidi O et al. 2018 Science & Sports 33 e141–e149.
- Schoenfeld BJ et al. 2016 European Journal of Sport Science 16 1–10.
- Schoenfeld B & Grgic J 2018 Strength & Conditioning Journal 40 107–112.
- Matsuo T et al. 2014 Medicine & Science in Sports & Exercise 46 42–50.
- Jelleyman C et al. 2015 Obesity Reviews 16 942–961.
- Garcia-Hermoso A et al. 2016 Obesity Reviews 17 531–540.
- Srikanthan P et al. 2016 American Journal of Cardiology 117 1355–1360.
- Srikanthan P & Karlamangla AS 2014 American Journal of Medicine 127 547–553.
- McGlory C et al. 2019 Journal of Physiology 597 1251–1258.


{kind=link}
{kind=link}
{kind=link}