Our Early Career Prize Lectures help early career scientists and clinicians have their work recognised across the wider endocrine community. Our 2021 Early Career Clinician Prize Lecturer presented at SfE BES 2021 in Edinburgh. Read on to learn more about their award-winning work. The application deadline for the 2022 Early Career Prize Lectures is 4 July 2022.
Up to 5% of adults and 10% of over 70-year-olds harbour an adrenal tumour. The vast majority of these tumours arise from the adrenal cortex, are benign, and do not cause specific clinical symptoms. Therefore, adrenal tumours are mostly discovered incidentally when carrying out a scan of the abdomen for unrelated reasons, prompting the use of the term ‘adrenal incidentaloma’.
Once an adrenal tumour is diagnosed, two crucial questions need to be answered to guide management:
- Is the tumour malignant?
Answering this question usually requires taking a detailed medical history (any previous history of extra-adrenal cancer?) and assessment of the imaging characteristics of the tumour, namely the size and the unenhanced computed tomography (CT) attenuation value of the tumour area.
- Is the tumour hormonally active?
This second question relies on physical examination and several hormonal tests to rule out excess production of cortisol, aldosterone, androgen precursors and catecholamines, all of which are produced by the adrenal glands. Cortisol excess is assessed by the 1mg dexamethasone overnight suppression test (1mg-DST).
MILD AUTONOMOUS CORTISOL SECRETION
'Our study is the largest ever to establish conclusively the extent of the risk and severity of hypertension and type 2 diabetes in patients with mild autonomous cortisol secretion.'
About 50% of benign adrenal tumours demonstrate evidence of hormone excess.
Clinically overt cortisol excess, also known as Cushing’s syndrome, is rare and typically presents with distinct clinical signs such as proximal myopathy and purple striae, but also with less specific metabolically adverse consequences, including type 2 diabetes, hypertension and dyslipidaemia.
Mild autonomous cortisol secretion (MACS) is far more common than Cushing’s syndrome. It is associated with up to one third of benign adrenal tumours, according to previous small-scale studies. However, patients usually show no characteristic clinical signs of Cushing’s syndrome. MACS is defined by failure to suppress serum cortisol sufficiently after overnight administration of 1mg dexamethasone in the 1mg-DST.
Several smaller-scale studies have suggested that MACS is potentially associated with frailty and an increased risk of mortality and cardiometabolic morbidities, including metabolic syndrome, cardiovascular events, atrial fibrillation and osteoporosis. Due to the high prevalence and potential clinical consequences of MACS, the joint guideline by the European Society of Endocrinology and the European Network for the Study of Adrenal Tumors (ENSAT) recommends that all patients with adrenal tumours should undergo a 1mg-DST.

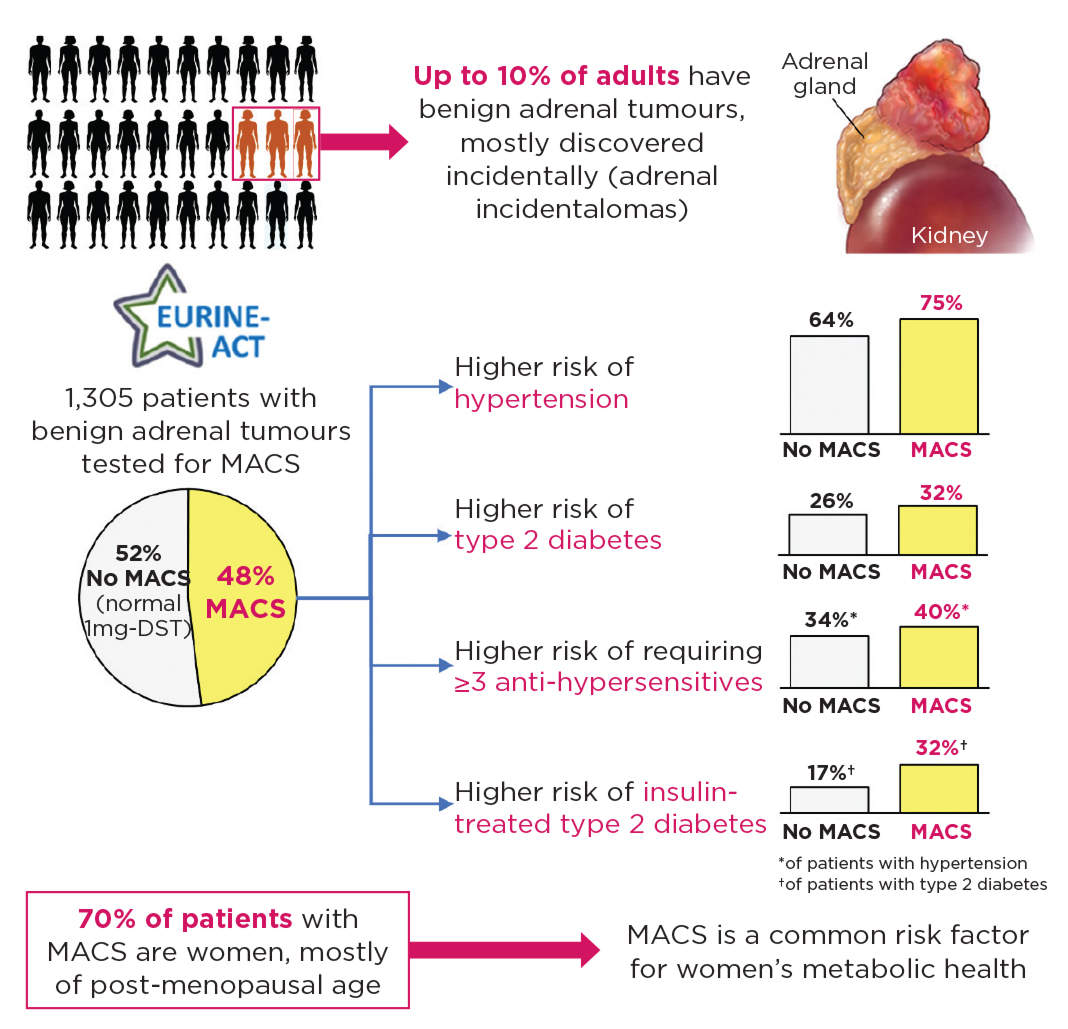
Figure. All patients with newly diagnosed adrenal tumours should undergo a 1mg-DST to screen for MACS. In the EURINE-ACT Study, 1,305 patients with benign adrenal tumours (incidentally discovered in 1,240) underwent a 1mg-DST. 48% of patients with adrenal incidentalomas had abnormal 1mg-DST results. Patients with MACS were more likely to be post-menopausal women and carried a higher cardiometabolic risk than those with normal 1mg-DST results.
THE EURINE-ACT STUDY
In 2011, the University of Birmingham started a large, prospective, multi-centre study on patients with newly diagnosed adrenal tumours: the Evaluation of Urine Steroid Metabolomics in the Differential Diagnosis of Adrenocortical Tumours (EURINE-ACT) Study. Over the course of 5 years, more than 2,000 participants were enrolled from 13 European and 1 American specialist ENSAT centres. This study was primarily designed to prospectively validate urine steroid metabolomics (USM), the combination of mass spectrometry-based steroid metabolome profiling and machine learning-based steroid data analysis. The EURINE-ACT Study results demonstrated that USM has superior specificity to imaging, and that the combination of unenhanced CT attenuation and USM provides the most sensitive and specific diagnostic information for detecting adrenocortical carcinoma.
However, more than 1,300 of the EURINE-ACT Study’s participants were diagnosed with benign adrenal adenomas and were tested for MACS with the 1mg-DST. This yielded the largest prospective cohort of this kind collected to date, and provided us with an excellent opportunity to investigate the impact of MACS on metabolic health in a very large, prospectively collected cohort. All patients underwent a detailed clinical assessment of their cardiometabolic risk and provided a 24-hour urine collection. The urine samples were analysed by multi-steroid profiling using tandem mass spectrometry to provide a detailed overview of adrenal steroid production and metabolism.
MACS, HYPERTENSION AND TYPE 2 DIABETES
It surprised us just how common MACS was: it was diagnosed in almost half the patients harbouring a benign adrenal incidentaloma. Notably, 70% of patients with MACS were women, and most of them were of postmenopausal age (over 50 years old).
Compared with those without MACS, we observed that patients with MACS were more likely to be diagnosed with hypertension and to require three or more anti-hypertensives to achieve adequate blood pressure control. When we looked at patients with a diagnosis of type 2 diabetes, those with MACS were twice as likely to be insulin-dependent, indicating that other medications have not helped in managing their blood sugar levels.
Examination of the steroids in the urine of patients with MACS, in comparison with those in subjects with normal 1mg-DST results, showed an increase in the excretion of cortisol and related metabolites. Conversely, the excretion of androgen metabolites was reduced in patients with MACS. Adrenal androgen production is stimulated by adrenocorticotrophin (ACTH); therefore, this observation is possibly linked to the negative feedback exerted by the cortisol excess on the pituitary, leading to reduced secretion of ACTH.
MACS: A VASTLY UNDERESTIMATED PROBLEM
Only a minority of patients with adrenal incidentalomas are referred to an endocrinologist and undergo optimal work-up to exclude MACS. Just one in six patients underwent a 1mg-DST in a recently published population-based study. If left undiagnosed, patients with MACS are at risk of developing adverse cardiometabolic consequences and presenting with poorly controlled hypertension and type 2 diabetes.
Based on our findings and the high prevalence of adrenal tumours, we estimate that up to 1.3 million adults in the UK could have MACS. Considering that around two out of three of these patients are women, MACS is potentially a key contributor to women’s metabolic health, particularly after menopause.
THE NEXT STEPS
Our study is the largest ever to establish conclusively the extent of the risk and severity of hypertension and type 2 diabetes in patients with MACS. We advocate that all patients with an adrenal incidentaloma are tested for MACS and, if MACS is confirmed, are regularly tested for type 2 diabetes and high blood pressure.
Going forward, our research will focus on three main areas. First, we want to investigate how MACS is linked to this increased risk by investigating how cortisol excess affects human metabolism. Secondly, we are working on a test that can be used at an early stage to identify which patients with MACS carry a higher risk of developing adverse cardiometabolic consequences. Thirdly, we are testing new treatment strategies to mitigate this risk in affected individuals.
Alessandro Prete
Diabetes UK Sir George Alberti Research Fellow, Institute of Metabolism and Systems Research, University of Birmingham
Wiebke Arlt
William Withering Chair of Medicine, and Director, Institute of Metabolism and Systems Research, University of Birmingham
FURTHER READING
- Prete A et al. 2022 Annals of Internal Medicine doi: 10.7326/M21–1737.
- Bancos I et al. 2020 Lancet Diabetes & Endocrinology 8 773–781.
- Elhassan YS et al. 2019 Annals of Internal Medicine 171 107–116.
- Kjellbom A et al. 2021 Annals of Internal Medicine 174 1041–1049.
- Ebbehoj A et al. 2020 Lancet Diabetes & Endocrinology 8 894–902.
- Bancos I & Prete A 2021 Journal of Clinical Endocrinology & Metabolism 106 3331–3353.
- Fassnacht M et al. 2016 European Journal of Endocrinology 175 G1–G34.



{kind=link}