Within the UK and most developed countries, we can categorically define our population as an ageing one. Current data suggest around 11 million people (19% of the population) are aged over 65, with this increasing to 13 million over the next decade.

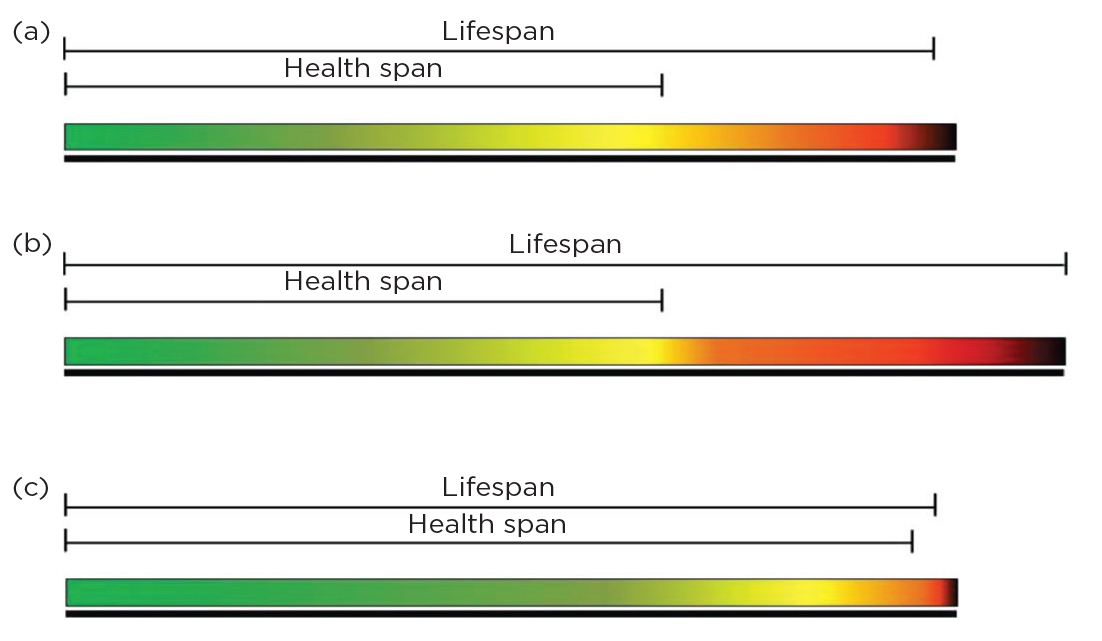
Figure 1. Differing approaches to treating populations of increasing age. Colours represent the relative health of an individual (green = good health ranging to dark brown = poor health). (a) The normal lifespan of an average person with reported years of poor health and disability. (b) A medical focus on lifespan extension only. (c) A medical focus on extension of health span only.10
Despite the average person living longer, the years for which we could expect to live in ‘good health’ have decreased to 62.4 years for men and 60.9 years for women. What these numbers tell us is that almost a fifth of the UK population is living in poor health due to age.1
Everyone faces an inevitable decline in their musculoskeletal health with increasing age, and this decline is heavily linked to poor health and disability. As patients with endocrine disease enter the later stages of life, they are more at risk of complications, particularly with musculoskeletal conditions. It is clear that, by focusing on age-related conditions, we could not solely extend lifespan, but increase health span for these individuals (Figure 1).2
COMMON MUSCULOSKELETAL AGEING PATHOLOGIES
Broadly, age-related changes to our musculoskeletal tissues can fall into three categories:
• muscle-based decline, called sarcopenia
• bone-based decline, usually related to osteoporosis, and
• joint-based conditions, such as arthritis.
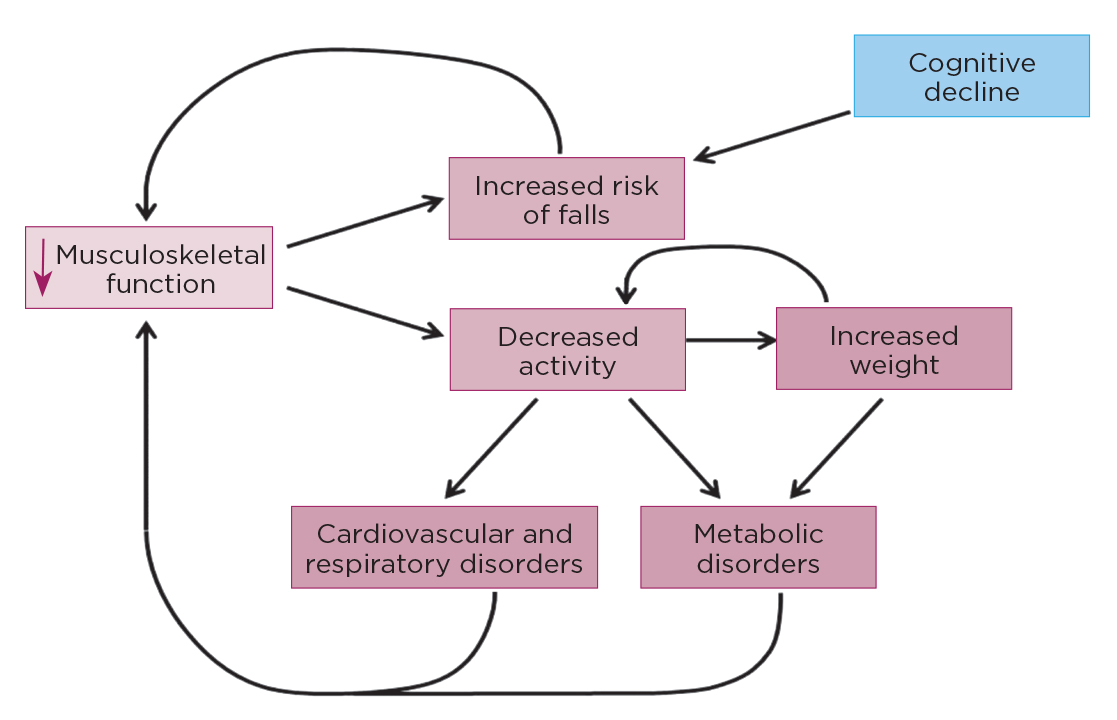
All of these conditions are inevitable to some degree, and everyone will suffer functional decline with increased age. Despite this, little progress has been made to counteract the loss. We can see the influence a loss of musculoskeletal function has for the whole-body system in Figure 2. For patients with underlying co-morbidities, the loss occurs to a higher extent and earlier in life, and therefore it is crucial to understand the impact of musculoskeletal loss here.3
In this article, I will focus on the impact endocrine diseases play in sarcopenia. Recent reviews of other conditions are available.4,5
SARCOPENIA

Figure 2. Placing musculoskeletal decline at the centre of age-related health decline. The decrease in musculoskeletal function can lead to increasing falls and decreasing activity, which feedback directly and indirectly, causing further declines. These effects are known to influence other age-related conditions and co-morbidities.
Sarcopenia is characterised by age-related decline in muscle mass and function. By the time a person reaches their 80s, they will have lost approximately 50% of their muscle mass.6 As muscle mass represents 60% of total body mass, this loss is clearly detrimental to each individual through reduced locomotion, strength and co-ordination, as well as alterations in metabolic processes.
Currently, the only way to avoid functional decline is to ensure you have developed more muscle mass in earlier life to hold off the functional deficit for longer. Treatments have focused on preserving the level of muscle mass a patient has through resistance training and diet, but this obviously doesn’t stop the decline.
We have seen in particular endocrine-related conditions that sarcopenia can be exacerbated. Potentially by studying these conditions, we can work backwards to understand the point of functional decline. At the very least, we can identify those groups that are more at risk of functional loss.
ENDOCRINE DISEASES AND SARCOPENIA
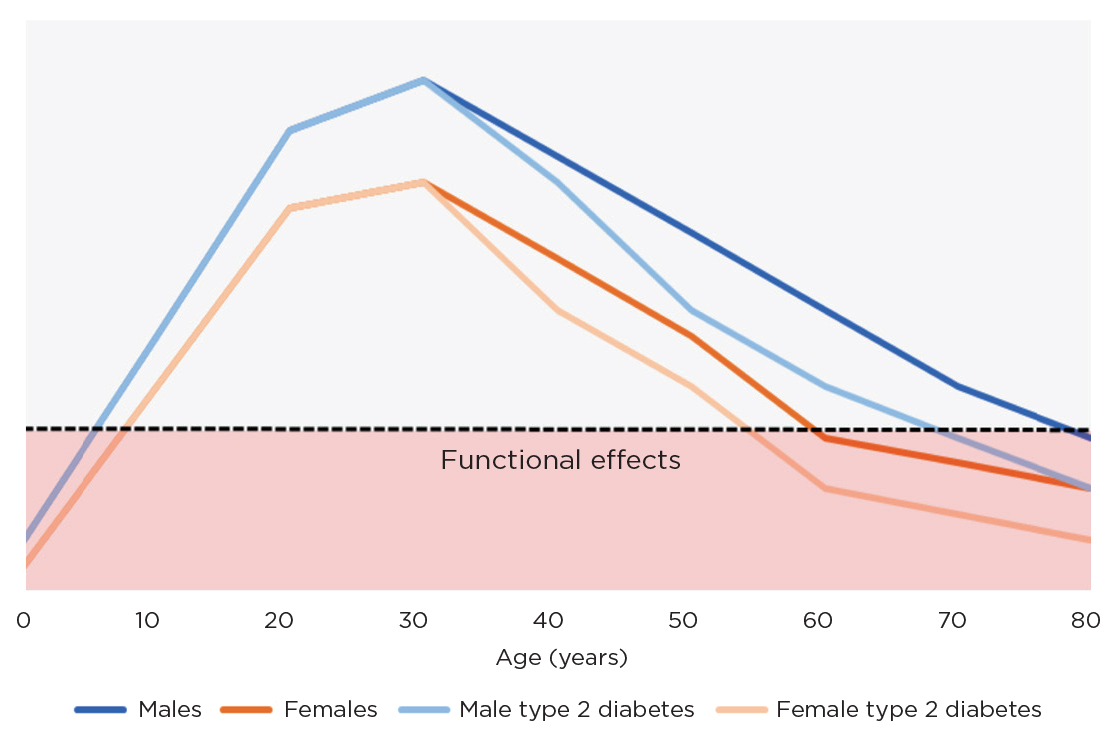
Sarcopenia has been described as a new complication of patients with type 2 diabetes, attributed in part to better care and management of the diabetes itself. In these patients, loss of muscle mass and function occurs earlier than in non-diabetic counterparts, with evidence of a decline in patients in their 50s and 60s. Type 2 diabetes is also strongly linked to increased frailty, disability and mortality.

Figure 3. Representative graph displaying the expected pattern of functional changes in skeletal muscle with increasing age for patients with and without type 2 diabetes. Any value below the functional effects line would probably display in patients as poor mobility or strength.
Ultimately, the more muscle mass that is lost in diabetic patients, the less capacity they have to dispose of glucose. In clinic, this would present as a higher glycated haemoglobin value (>8.5%) with decreased muscle mass. Whether the loss of muscle mass comes first, or the diabetes influences the reduction of muscle mass, is not currently known. However, it is clear that, in our older population of diabetics, special attention should be paid to any presentation of sarcopenia (Figure 3).7
Cushing’s syndrome is clinically defined by muscle weakness. Glucocorticoids have been shown to influence muscle structure through a loss of type II muscle fibres. Excess cortisol has additionally been shown to impair muscle protein synthesis and mitochondrial function. Despite studies showing that muscle and fat levels were similar in comparison groups, patients with Cushing’s syndrome display far less muscle function, due to higher levels of fat infiltration into the muscle tissue. This functional loss can last for more than two years after treatment, which can be highly detrimental in populations already displaying loss of muscle mass and function.8
Thyroid hormones have a role in the regulation and expression of over 600 genes in muscle tissue, through their involvement in energy production and metabolism. The presence of hyperthyroidism increases the turnover of protein in muscle tissues, ultimately leading to loss of muscle mass. A number of studies have shown high levels of muscle mass decline and loss of strength in patients with hyperthyroidism.8
In just these few examples, it is clear that recognising the development of sarcopenia in patients with underlying endocrine conditions is of huge importance for that patient’s long term health and well-being. Although we may not be able to prevent the decline in mass and function, we can look to commence suitable treatments in these populations earlier, to ensure function is maintained for as long as possible.
SARCOPENIA AND THE MENOPAUSE
'Use of HRT in the initial postmenopausal period results in significant increases in muscle stem cells, strength and mobility.'
The incidence and impact of musculoskeletal conditions are highly sex-specific. Sarcopenia is intimately linked with the female ageing process. One of the most influential times in a women’s life is when she reaches the menopause, which brings about huge physiological change, particularly in endocrinology.
One of the more potent hormonal changes that is displayed is in the levels of the oestrogen hormone oestradiol. This hormone is involved in the regulation of the menstrual cycle and in the development of female sexual characteristics but is relevant to muscle, as muscle fibres contain specific receptors for oestradiol. Oestradiol therefore has a role in muscle function, specifically in stimulating the muscle stem cells to grow and divide, to promote muscle growth.9
Without oestradiol present in the system, muscle cells will be unable to repair and replace damaged fibres. Over time, this leads to a culminative loss of mass and function at an accelerated rate. In this situation, we do see some slowing down of the muscle loss with hormone replacement therapies (HRT), but its power comes from quick implementation. Use of HRT in the initial postmenopausal period results in significant increases in muscle stem cells, strength and mobility when compared with HRT introduced in a delayed postmenopausal period.
The ongoing debate on the risks associated with HRT will prevent this from being a universal approach to sarcopenia but, if we can focus on commencing HRT as soon as possible in those who are suitable, we can begin to make a substantial difference to people.
SUMMARY
Sarcopenia, as with other age-related musculoskeletal diseases, is inevitable for all of us. However, for those with underlying conditions, such as the ones discussed, it can develop sooner and have a greater impact on the individual.
Individuals with endocrine disease should be monitored for evidence of musculoskeletal decline, to prevent the early onset of loss of functionality which, in turn, can negatively impact their conditions.
Simple advice and education regarding the conditions, and introducing resistance exercise and nutritional approaches, may well make the difference. However, as our ability to treat and manage endocrine disease improves, we may soon be faced with a range of age-related effects of endocrine disease that we have never considered before.
GARETH NYE
Senior Lecturer of Anatomy and Physiology, University of Chester
REFERENCES
1. Office for National Statistics 2021 Census 2021.
2. Kirkland JL & Peterson C 2009 Journals of Gerontology, Series A, Biological Sciences & Medical Sciences 64 209–212.
3. Buford TW et al. 2010 Ageing Research Reviews 9 369–383.
4. Cannarella R et al. 2019 Journal of Clinical Medicine 8 1564.
5. Bertoldo E et al. 2021 Frontiers in Endocrinology 12 620920.
6. Faulkner JA et al. 2007 Clinical & Experimental Pharmacology & Physiology 34 1091–1096.
7. Izzo A et al. 2021 Nutrients 13 183.
8. Morley JE 2017 Current Pharmaceutical Design 23 4484–4492.
9. Geraci A. et al. 2021 Frontiers in Endocrinology 12 682012.
10. Blagosklonny MV 2012 Aging 4 547–552.



{kind=link}
{kind=link}
{kind=link}