Loss of endocrine function of the ovaries, with resultant absolute deficiency of female sex steroids, is typically associated with ageing. If this happens before the age of 40 years, this is defined as premature ovarian insufficiency.
The prevalence of POI is around 1–3%.1 In most cases, the cause of POI is unexplained. Around 30% of patients will have an underlying genetic condition, with Turner syndrome and Fragile X being the most common. Other cases are associated with gonadotoxic chemotherapy or radiotherapy, or surgery for malignant or benign disease. Almost all female patients with galactosaemia will have POI.
Women with POI present with primary or secondary amenorrhoea; primary amenorrhoea is more common in those with a genetic cause. A diagnosis of POI is made based on menstrual disturbance (absent or infrequent irregular periods) and follicle-stimulating hormone (FSH) being raised beyond physiological levels (>25–30IU/l) on two occasions, taken a minimum of 4–6 weeks apart.2 In a minority of cases, the diagnosis will be self-evident, with a history of surgical removal of both ovaries.
NICE,3 the International Menopause Society,4 the European Society of Human Reproduction and Embryology2 and the British Menopause Society5 have all published guidelines covering the diagnosis and management of POI.
HEALTH IMPACT OF POI
Untreated oestrogen deficiency has a significant impact on quality of life. Most women report bothersome menopausal symptoms including hot flushes, sleep disturbance, mood disturbance, or vulvo–vaginal dryness and discomfort.
Epidemiological studies have also consistently shown an association between untreated POI and increased risk of osteoporosis and fracture6 and heart disease.7 One cohort study of women with surgical menopause has even shown an association with cognitive impairment and dementia.8
CHOICE OF HORMONE THERAPY
All guidelines recommend treatment with either hormone replacement therapy (HRT) or the combined oral contraceptive (COC) until the average age of natural menopause (51 years of age) to maintain health.2–5
Although POI is associated with infertility, around 5–10% of women with POI can conceive spontaneously, due to fluctuating ovarian activity. If contraception is needed, the COC inherently provides contraceptive cover. Alternately, an HRT regimen incorporating the Mirena coil or with the addition of the progestogen-only pill can be used.
'The POISE trial aims to find the relative effectiveness of HRT (any route) compared with the combined oral contraceptive in individuals with POI.'
The COC is often seen as more acceptable to young people and is free of prescription charges. It is recommended that a COC with 30μg ethinyloestradiol and progestogen is prescribed as an extended regimen (tricycling for 63 days followed by a 4–7 day interval, or flexible extended use, taking it continuously with breaks of 3–4 days if breakthrough bleeding occurs). Using the COC in these ways minimises the number of days without oestrogen exposure.
HRT is generally prescribed in secondary care and comes in a variety of formulations with different routes, doses and commercial availability. The recommended daily dose of oestradiol for POI is not less than 2mg orally, a 50μg patch or 1.5mg gel. This dose can be titrated upwards if needed for symptoms or to maintain bone density.
Women should be reassured that, unlike HRT use after the average age of menopause, the incidence of breast cancer is not higher than that of the general population in those using HRT <40 years of age.9
Little evidence is available to support patients and clinicians in choosing between HRT and the COC to maintain health.
A small randomised controlled trial suggests that blood pressure is lower in HRT users than in COC users;10 however, the clinical significance of this in isolation is unclear. A larger randomised controlled trial suggests that bone mineral density is higher in HRT users than in COC users,11 but this alone has not been sufficient to change practice.

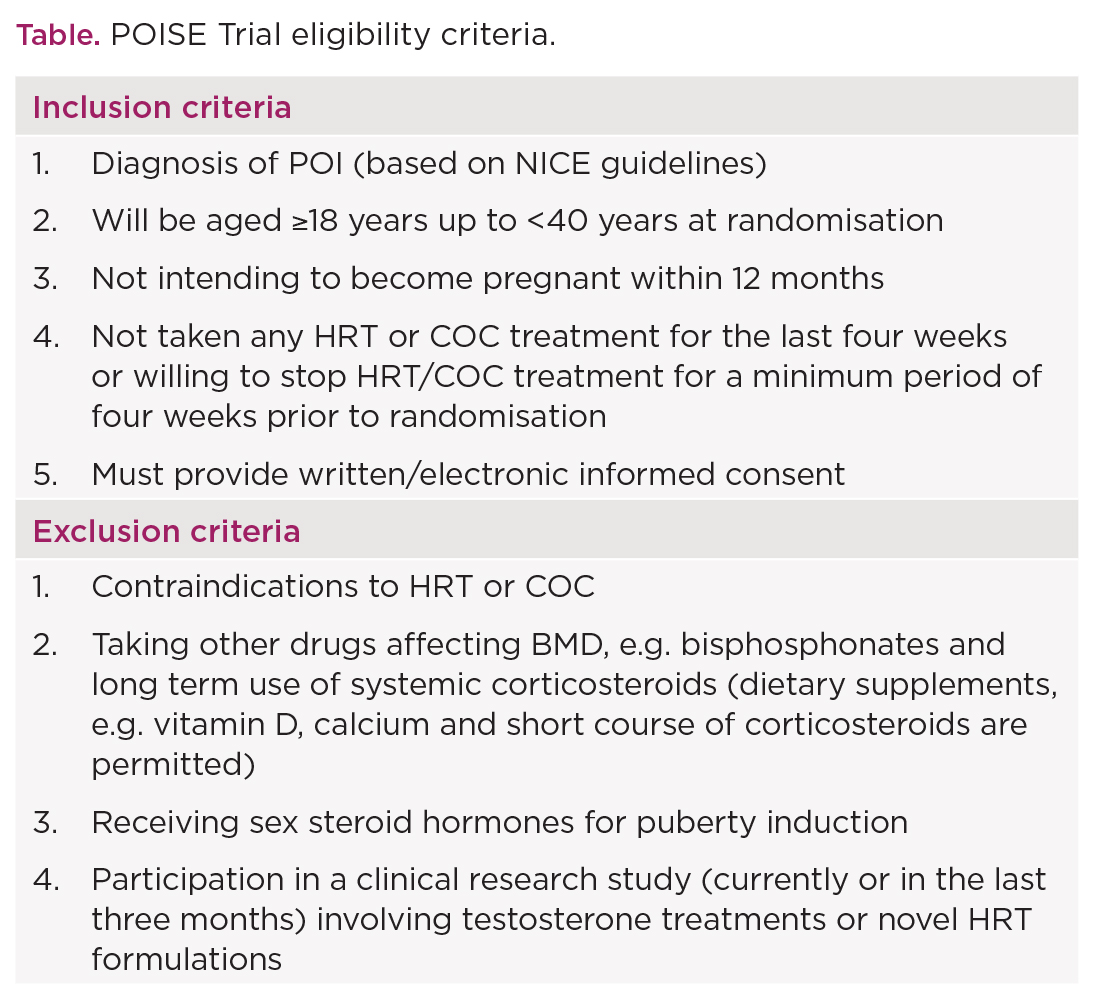
Table. POISE Trial eligibility criteria.
Adding testosterone to adequate HRT does not appear to further increase bone mineral density (BMD), and its use should be restricted to cases with POI and low sexual desire who are seen in a specialist setting.2
POISE TRIAL
The POISE Trial is funded by the NIHR Health Technology Assessment Programme. It aims to find the relative effectiveness of HRT (any route) compared with the COC in individuals with POI.
The primary outcome is the absolute BMD (g/cm2) of the lumbar spine at two years from randomisation, assessed by a dual-energy X-ray absorptiometry scan. Secondary outcomes include menopause-specific quality of life, sexual function, work productivity, and satisfaction with treatment. In a small number of sites, participants are asked to provide blood and urine samples for biomarker analysis. Consent is also obtained for long term follow up using routine data.
With support from The Daisy Network, a charity for women with POI, and the Turner Syndrome Support Society, the POISE Trial aims to recruit 480 women with POI across 24 centres around the UK. Recruitment began in June 2022 and will continue for 36 months. The POISE Trial eligibility criteria are outlined in the Table.
ZACHARY NASH
Clinical Research Fellow in Gynaecology, EGA Institute for Women’s Health, University College London
MELANIE DAVIES
Professor of Reproductive Medicine, EGA Institute for Women’s Health, University College London; Chief Investigator, the POISE Trial (NIHR128757)
REFERENCES
1. Golezar S et al. 2019 Climacteric 22 403–411
2. Webber L et al. 2016 Human Reproduction 31 926e37.
3. NICE 2015 Menopause: Diagnosis and Management NG23.
4. Panay N et al. 2020 Climacteric 23 426e46.
5. Hamoda H et al. 2017 Post Reproductive Health 23 22–35.
6. Sullivan SD et al. 2015 Menopause 22 1035–1044.
7. Zhu D et al. 2019 Lancet Public Health 4 E553–E564.
8. Rocca WA et al. 2007 Neurology 69 1074–1083.
9. Collaborative Group on Hormonal Factors in Breast Cancer 2019 Lancet 394 1159–1168.
10. Langrish JP et al. 2009 Hypertension 53 805–811.
11. Cartwright B et al. 2016 Journal of Clinical Endocrinology & Metabolism 101 3497–3505.


{kind=link}