The hormone oxytocin is important for social interaction, is involved in emotion regulation and has anxiolytic properties. Researchers from the University Hospital of Basel (Switzerland) have succeeded in demonstrating a clinically relevant deficiency of oxytocin in patients with vasopressin deficiency (AVP deficiency or central diabetes insipidus). This finding could be key to developing new therapeutic approaches.
CURRENT UNDERSTANDING FROM RESEARCH
Even though the hormones oxytocin and vasopressin are both produced in the same hypothalamic area and are almost similar in structure, they have different functions in the body (Figure 1). Vasopressin is the main endocrine regulator of renal water excretion, and maintains fluid balance by keeping plasma volume and osmolality within narrow limits.1 The main function of oxytocin is to promote prosocial effects such as in-group favouritism, trust and attachment. It increases empathy, improves emotion recognition and has anxiolytic effects.2
Disruption of the hypothalamic–pituitary area can cause a deficiency of vasopressin, known as central diabetes insipidus, which is clinically characterised by polyuria and polydipsia.1 Despite treatment with desmopressin (a vasopressin receptor 2 agonist), patients often report residual psychological symptoms. The available studies in these patients have suggested heightened anxiety and difficulties describing or expressing emotions, reduced empathic abilities, higher levels of self-reported autistic traits, lower levels of joy when socialising, and lower scores in an emotion recognition task.3–6

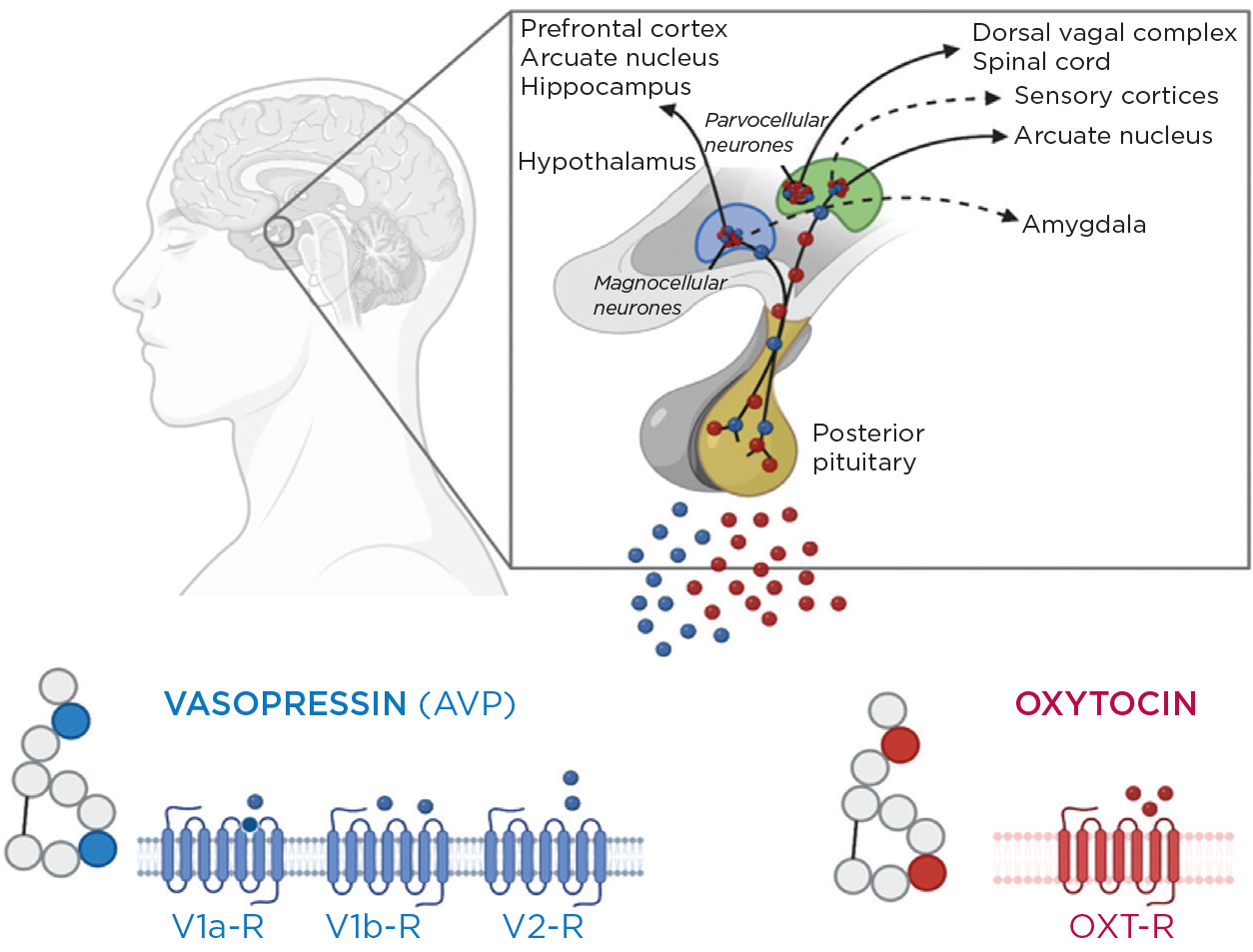
Figure 1. Hypothalamic–posterior pituitary axis. Vasopressin and oxytocin are both produced in the hypothalamic supraoptic and paraventricular nuclei, stored and released into the circulation from the posterior pituitary. biorender.com
Due to the anatomical proximity, disruptions leading to vasopressin deficiency could also affect oxytocin-producing neurones. An additional oxytocin deficiency in these patients could explain – at least partially – the observed socio-emotional and psychological changes. Few studies have attempted to measure oxytocin in these patients, delivering inconclusive results.4,7 For other pituitary hormones, a provocation test is often applied in case of a suspected deficiency. So far, however, no standard provocation test for oxytocin has been established to prove this disease entity.
NOVEL OXYTOCIN PROVOCATION TEST
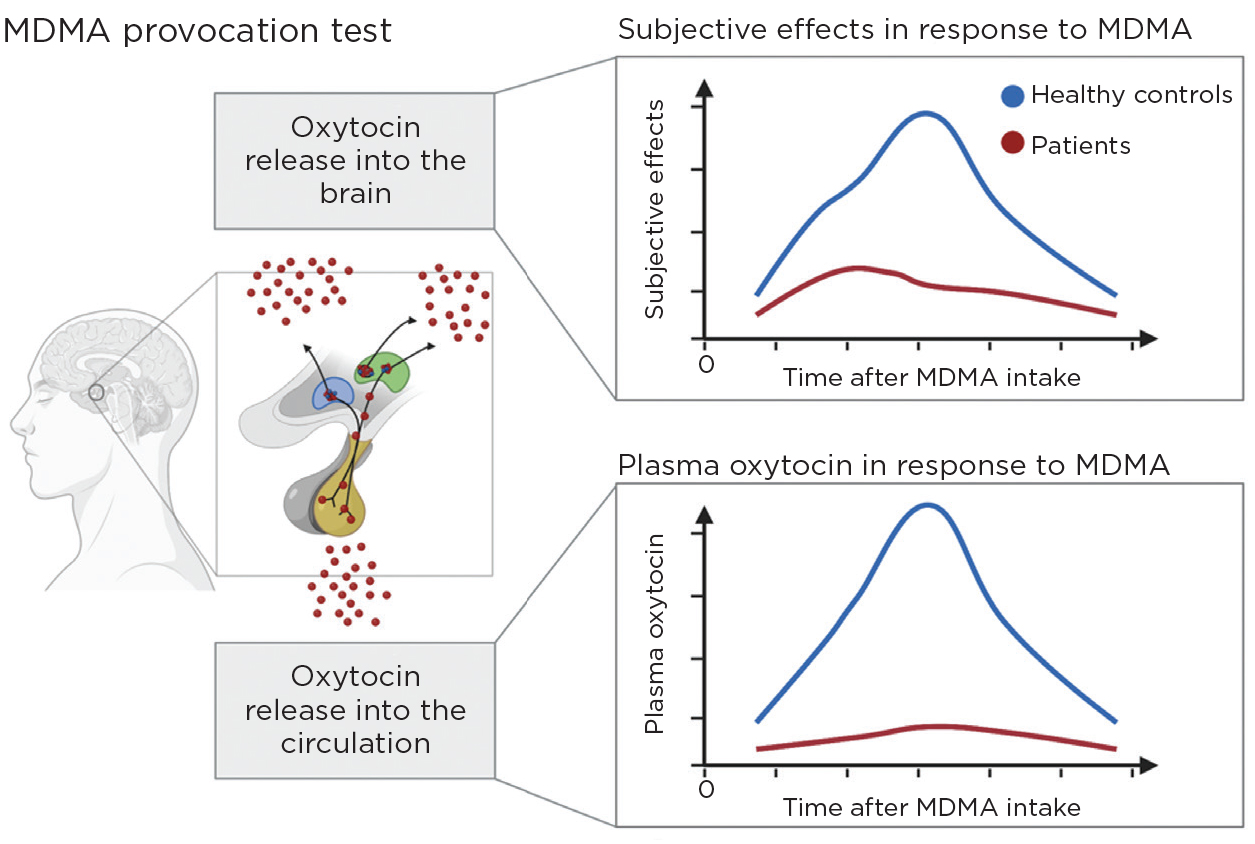
Methylenedioxymethamphetamine (MDMA, also known as ‘ecstasy’) is used recreationally for its effects on empathic feelings and sociability. Several studies have documented marked increases in circulating oxytocin levels in response to MDMA in healthy adults.8,9 The prosocial effects of MDMA on emotion processing and social interaction, such as increased trust, closeness to others, identification of facial emotions, and fear extinction, are mediated partly by a strong oxytocin release.9
Using MDMA (‘ecstasy’) as a psychoactive and biochemical provocation test, our recent study has, for the first time, indicated a clinically relevant oxytocin deficiency in patients with vasopressin deficiency.10 In healthy controls, there was an expected eightfold increase in plasma oxytocin from 77pg/ml (interquartile range (IQR) 59–94) at baseline by 659pg/ml (IQR 355–914) in response to MDMA stimulation, with typical prosocial, empathic and anxiolytic subjective effects. In contrast, in patients, no notable increase was observed, and plasma oxytocin only slightly increased from 60pg/ml (IQR 51–74) by 66pg/ml (IQR 16–94). In agreement with the lack of oxytocin increase, lower MDMA-induced subjective effects such as ‘trustful feelings’, ‘closeness to others’ or ‘happiness’ were observed, reflecting a lack of activation of central key regions important for socio-emotional processing (Figure 2).

Figure 2. Schematic illustration of the study results. biorender.com
Furthermore, in response to MDMA, healthy controls demonstrated reduced recognition of negative emotions (i.e. ‘anger’, ‘fear’ and ‘sadness’) in the emotion recognition task, increased empathy for positive emotions, and reported anxiolytic effects. In contrast, in patients, there was no reduced recognition of ‘fearful’ emotions, no increase in empathy, and no anxiolytic effect. In particular, the lack of increase in ‘positive empathy’ (the ability to share, celebrate and enjoy others’ positive emotions, a state which correlates with increased prosocial behaviour, social closeness and well-being) might contribute to the psychological findings observed in the study.
TREATMENT WITH OXYTOCIN?
These results provide strong evidence for a clinically relevant oxytocin deficiency in patients with vasopressin deficiency. This finding opens up new therapeutic possibilities. The effects of oxytocin administration in patients with vasopressin deficiency have only been reported in one small study, demonstrating an improvement in the previously impaired ability to categorise negative emotions after a single dose of intranasal oxytocin.11 Future studies in a larger patient population should investigate the potential therapeutic use of intranasal oxytocin.
The same group at the University Hospital of Basel is currently planning a large study to investigate whether treatment with oxytocin can improve the psychological symptoms in patients with vasopressin deficiency.
CIHAN ATILA
Clinical Scientist, University Hospital Basel, Department of Endocrinology, Diabetes and Metabolism, Department of Clinical Research, Basel, Switzerland
MIRJAM CHRIST-CRAIN
Full Professor in Endocrinology, Co-Head of the Department of Clinical Research and Deputy Head of the Department of Endocrinology, University Hospital Basel, Department of Endocrinology, Diabetes and Metabolism, Department of Clinical Research, Basel, Switzerland
REFERENCES
- Christ-Crain M et al. 2019 Nature Reviews Disease Primers 5 54.
- Meyer-Lindenberg A et al. 2011 Nature Reviews Neuroscience 12 524–538.
- Atila C et al. 2022 Lancet Diabetes & Endocrinology 10 700–709.
- Aulinas A et al. 2019 Journal of Clinical Endocrinology & Metabolism 104 3181–3191.
- Brandi ML et al. 2020 Journal of Neuroendocrinology 32 e12842.
- Gebert D et al. 2018 Psychoneuroendocrinology 88 61–69.
- Sailer CO et al. 2021 European Journal of Endocrinology 185 355–364.
- Holze F et al. 2020 Neuropsychopharmacology 45 462–471.
- Hysek CM et al. 2012 Psychopharmacology 222 293–302.
- Atila C et al. 2023 Lancet Diabetes & Endocrinology 11 454–464.
- Hoffmann A et al. 2017 Endocrine 56 175–185.


{kind=link}
{kind=link}
{kind=link}