The first question you may ask is ‘Why are we discussing non-alcoholic steatohepatitis (NASH) in The Endocrinologist?’ Fatty liver (steatosis) is found in 15–30% of the adult population. The commonest cause is insulin resistance, which is associated with metabolic syndrome and type 2 diabetes. An accumulating body of evidence links adipose tissue expandability defects and inflammation with non-alcoholic fatty liver disease (NAFLD); the metabolic milieu (glucose and insulin) drives enhanced de novo lipogenesis within hepatocytes and the accumulation of lipotoxic intermediates, thereby exacerbating liver damage.
WHAT ARE THE TERMINOLOGY, DIAGNOSIS AND CONSEQUENCES?
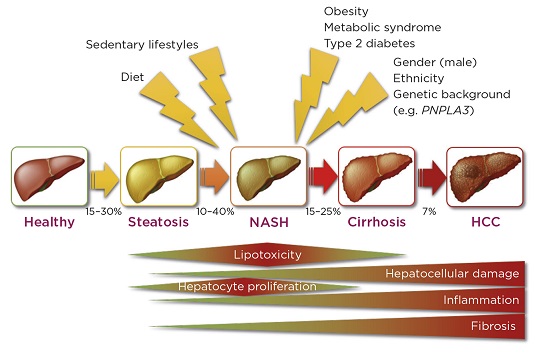
NAFLD is the term describing the whole spectrum of this condition. Steatosis describes simple fat accumulation within hepatocytes, whereas NASH refers to the presence of fat associated with inflammatory infiltrates and fibrosis (see Figure).
Differentiating between ‘benign’ steatosis and NASH remains difficult. Despite extensive work on imaging tools and non-invasive biomarkers, the gold standard continues to be liver biopsy. Natural history data indicate that NASH, as opposed to steatosis, can progress to advanced liver disease, with risk of liver cancer and liver failure necessitating liver transplantation. The relevance of NASH as a cause of cirrhosis is demonstrated by the fact that NASH-related cirrhosis will soon become the commonest indication for liver transplantation.

Stages and pathophysiology of NASH (HCC, hepatocellular carcinoma). ©M. Allison & M. Vacca
DOES YOUR PATIENT HAVE SIGNIFICANT LIVER DISEASE?
Given the prevalence of NAFLD in the population, one of the major challenges is determining who has NASH with significant fibrosis. A number of staging algorithms based on blood tests and simple clinical parameters have been developed with this in mind, but those currently available are imperfect.
Simple tools such as FIB-4 (Fibrosis-4) or the NAFLD Fibrosis Score, which incorporate factors such as age, AST (aspartate aminotransferase), ALT (alanine aminotransferase) and platelet count, as well as the presence/absence of diabetes or impaired glucose tolerance, have been found to be most useful as a means of excluding significant NASH in patients with a score below a defined threshold. Additional methods of assessing individuals within the NAFLD spectrum include imaging modalities determining liver stiffness, most commonly using transient electrography (e.g. Fibroscan); this correlates with the amount of fibrosis.
Experts in the field recommend focusing on patient groups at high risk of significant liver disease, rather than assessing people based on the abnormality of liver function tests. Patients with diabetes are at significant risk of having active NASH with progressive fibrosis, as well as a twofold increased risk of liver cancer. As such, assessment of liver disease should be introduced into the regular assessment of type 2 diabetic patients in the same way that other comorbidities (e.g. retinopathy, neuropathy and nephropathy) are routinely assessed. Close links between primary and secondary care diabetes services and hepatology services, and shared pathways for the management of these subjects, are thus highly recommended.
IS THERE AN EFFECTIVE TREATMENT?
Weight reduction achieved through programmes of lifestyle revision or bariatric surgery is the most effective treatment in NASH. There is a good rationale for the pharmacological management of the underlying metabolic disease (including insulin sensitisers like metformin or pioglitazone, and liraglutide) and antioxidants (e.g. vitamin E), but no generally accepted treatment to improve liver histology in the long term. Although controversial, we believe that insulin therapy should be reserved for late stage diabetes if NASH coexists, to avoid excessive hepatic lipogenesis.
Having previously been a frustrating area to treat, long term phase 3 studies are currently being undertaken to examine the effectiveness of agents including other glucagon-like peptide-1 receptor agonists, farnesoid X receptor agonists, peroxisome proliferator-activated receptor (PPAR) α/δ agonists, and anti-inflammatory and anti-fibrotic drugs. In addition, other molecules in earlier phase studies are targeting metabolic and inflammatory processes. This rapidly changing landscape means that it will be increasingly important to diagnose/stage NASH.
Michael Allison, NASH Service, Liver Unit, Cambridge Biomedical Research Centre, Addenbrooke’s Hospital, Cambridge, UK
Michele Vacca, NASH Service, Liver Unit, Cambridge Biomedical Research Centre and Lipid Service, Addenbrooke’s Hospital, Cambridge, and Department of Biochemistry and Institute of Metabolic Science, University of Cambridge, UK


{kind=link}