Back in 1996, a research team led by Danny Welch at the University of Pennsylvania (Hershey, PA, USA) first identified the kisspeptin gene (KISS1) for its anti-metastatic properties in malignant melanoma.1 Little did they know that, over 20 years later, kisspeptin would be positioning for the role of master regulator of reproduction.

Figure 1. Hershey’s Kisses, the chocolates that gave their name to kisspeptin. ©A Comninos and W S Dhillo
They named it after the most famous local product from their university campus town in Hershey: the chocolates called ‘Hershey’s Kisses’ (Figures 1 and 2). It seems therefore somewhat appropriate that kisspeptin, containing as it does the word ‘kiss’, would several years later emerge as a key hormone in reproduction.
REVEALING KISSPEPTIN’S ROLE
It was in 2003, 7 years after the initial discovery of kisspeptin, that its crucial roles in reproduction began to emerge. Two large consanguineous families (from France and Saudi Arabia) had sought medical review for infertility. Five of the eight children in the French family and six of the nineteen children in the Saudi Arabian family were diagnosed with infertility due to hypogonadotrophic hypogonadism.2,3

Figure 2. A visit to the Hershey’s chocolate factory in Pennsylvania. ©A Comninos and W S Dhillo
Mutation analyses revealed inactivating mutations in the kisspeptin receptor gene. Subsequent studies demonstrated that inactivating mutations in the kisspeptin gene itself also resulted in hypogonadotrophic hypogonadism,4 while, conversely, activating mutations resulted in central precocious puberty.5 Hence, the stage was set for an explosion of interest in exploring the roles of kisspeptin in reproduction.
THE APEX OF THE AXIS
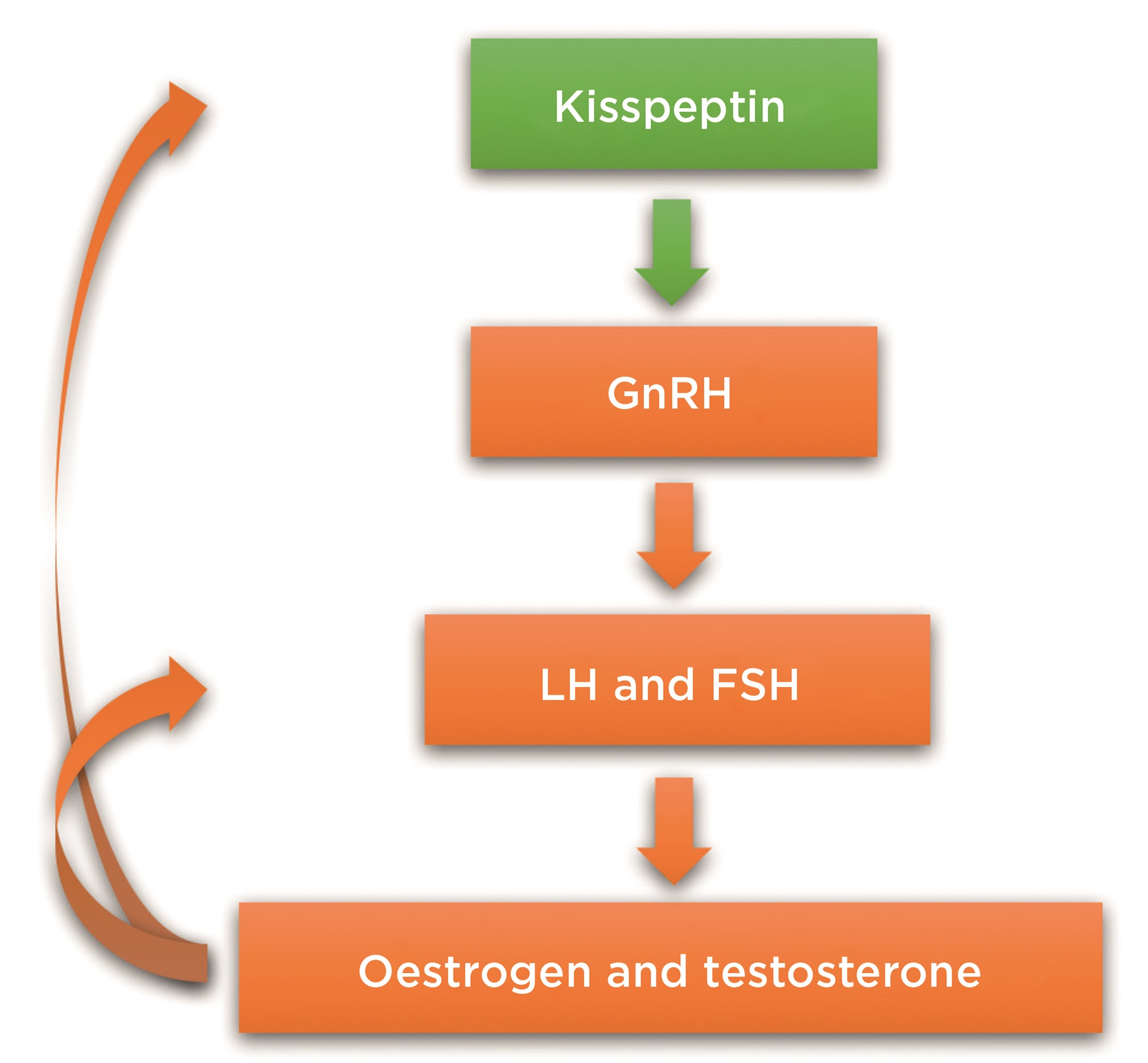
It soon emerged that kisspeptin is positioned at the apex of the reproductive axis (Figure 3). Kisspeptin is secreted by specialised kisspeptin neurones within the hypothalamus. It activates kisspeptin receptors upon gonadotrophin-releasing hormone (GnRH) neurones, resulting in downstream stimulation of reproductive hormone release (luteinising hormone, follicle-stimulating hormone, testosterone and oestradiol). This ability of kisspeptin to stimulate downstream reproductive hormones was demonstrated in man in 2005 by the first kisspeptin into human study.6

Figure 3. Kisspeptin sits at the apex of the reproductive axis (GnRH, gonadotrophin-releasing hormone; LH, luteinising hormone; FSH, folliclestimulating hormone). ©A Comninos and W S Dhillo
The ability of kisspeptin to regulate reproductive hormones was studied in earnest over the next decade in a variety of species (from zebrafish to humans).7,8 These studies revealed that kisspeptin neurones integrated with a variety of other hormones and neuropeptides, including prolactin, leptin, pro-opiomelanocortin, neuropeptide Y, vasopressin, oxytocin, GABA (γ-amino-butyric acid), glutamate, nitric oxide, neurokinin B, dynorphin, serotonin and dopamine. This placed kisspeptin in the centre of a web, orchestrating the reproductive, metabolic and behavioural control of reproduction.
Indeed, the mechanism whereby hyperprolactinaemia shuts down the reproductive axis is now believed to occur via prolactin receptors on kisspeptin neurones.9,10 Similarly, positive and negative gonadal feedback on GnRH neurones also occurs predominantly via kisspeptin neurones, as GnRH neurones themselves lack the oestrogen receptor-β required for feedback. GnRH neurones also lack leptin receptors – the effects of leptin on reproduction are executed via kisspeptin neurones.11 Further roles for kisspeptin in circadian reproductive systems, including puberty initiation, mid-cycle luteinising hormone surge and seasonal reproduction, were soon identified.

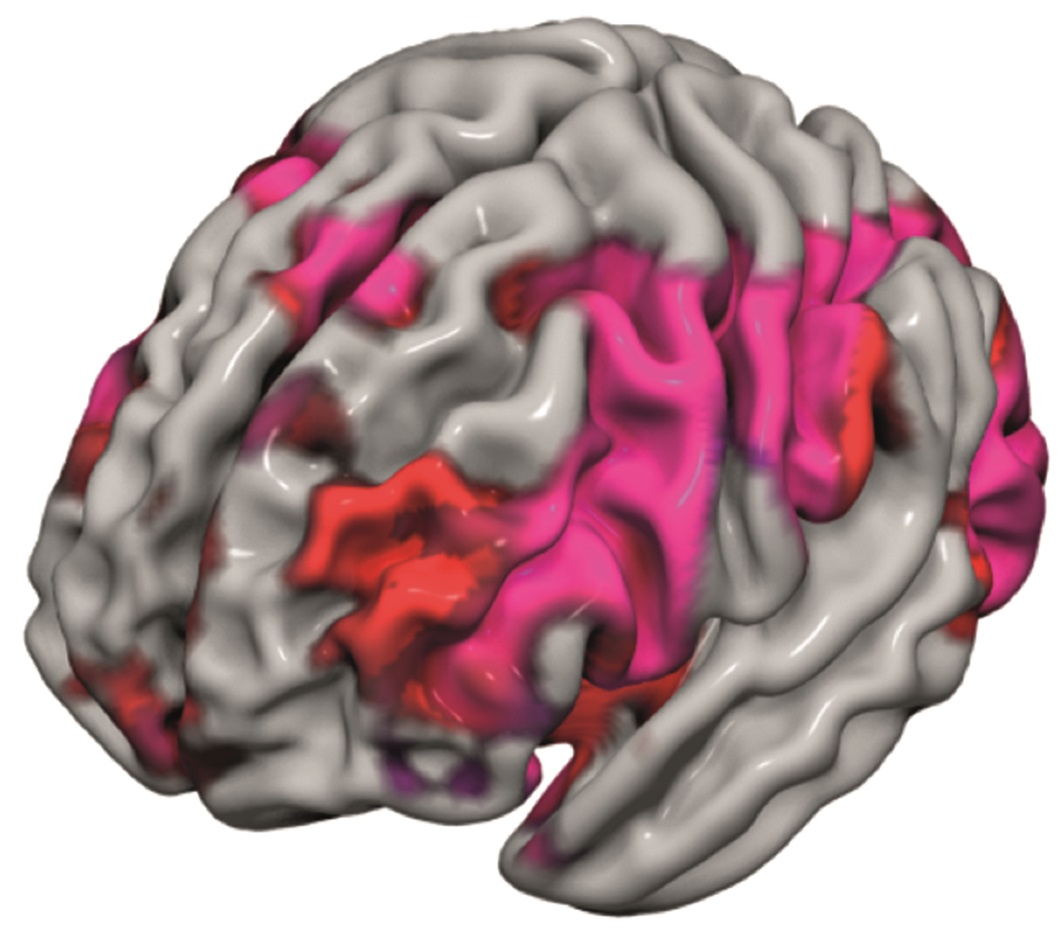
Figure 4. Kisspeptin enhances sexual and emotional brain processing. ©A Comninos and W S Dhillo
A ROLE IN BEHAVIOUR
Interestingly, kisspeptin signalling also occurs in key behavioural (e.g. limbic) structures of the brain and can influence reproductive hormone release.12 With this finding, we became particularly interested in how kisspeptin may modulate human behavioural processing encompassing sex and emotions.
Using functional magnetic resonance imaging and a range of psychometric methods, we found that kisspeptin could enhance human limbic brain activity specifically when men viewed sexually stimulating images as well as non-sexual images of couples bonding (Figure 4). Furthermore, kisspeptin’s ability to enhance limbic brain activity correlated with reward metrics, improved mood and reduced sexual aversion.13
Our human data, combined with studies in animals,14–17 therefore suggest that kisspeptin can also modulate sexual and emotional processing, thereby integrating these with reproduction, perhaps to ensure survival of the species, or at least contributing to an urge for sexual activity. This opens up the exciting possibility that kisspeptin-based therapies may help patients with psychosexual dysfunction
ROLES BEYOND THE BRAIN
Kisspeptin also has roles in reproductive tissues beyond the brain, with studies implicating kisspeptin signalling in ovarian and uterine function, embryo implantation and placentation, as well as in testicular and sperm function.18 Therefore, kisspeptin modulates not only central reproductive effects, but also acts directly on reproductive organs.
LOOKING TO THE FUTURE
Danny Welch and colleagues in 1996 surely had no idea that, two decades after identifying the kisspeptin gene for its anti-metastatic effects, kisspeptin would be the subject of such excitement in the field of reproduction. Nearly 2,000 papers have been published since then, collectively demonstrating the crucial and multi-faceted roles of kisspeptin.
Indeed, last year, together with other kisspeptin researchers, we organised the 3rd World Kisspeptin Conference in Orlando (FL, USA), which was perhaps the equivalent of a ‘Kisspeptin Disney World’ such was the academic excitement experienced by all!
One particular area of excitement is how we can develop this basic, translational and clinical kisspeptin research into practice, for the benefit of our patients. In beginning to answer this, several studies have demonstrated that kisspeptin-based therapies may have a role in idiopathic hypogonadotrophic hypogonadism, hypothalamic amenorrhoea, hyperprolactinaemia, in vitro fertilisation, polycystic ovarian syndrome and psychosexual disorders.10,13,19,20 Translating these possibilities into routine clinical use will be the challenge for the next decade of kisspeptinology.
So is kisspeptin, indeed, the master regulator of reproduction? Certainly, its newly identified roles in reproductive hormone and organ control, feedback mechanisms and integration with metabolism, as well as in sexual and emotional behaviours, would suggest it may indeed be precisely that.
Alexander N Comninos, Consultant Endocrinologist and Honorary Senior Lecturer, Imperial College Healthcare NHS Trust and Imperial College London
Waljit S Dhillo, Professor of Endocrinology and Metabolism, Imperial College London
REFERENCES
- Lee JH et al. 1996 Journal of the National Cancer Institute 88 1731–1737.
- de Roux N et al. 2003 Proceedings of the National Academy of Sciences of the USA 100 10972–10976.
- Seminara SB et al. 2003 New England Journal of Medicine 349 1614–1627.
- Topaloglu AK et al. 2012 New England Journal of Medicine 366 629–635.
- Silveira LG et al. 2010 Journal of Clinical Endocrinology & Metabolism 95 2276–2280.
- Dhillo WS et al. 2005 Journal of Clinical Endocrinology & Metabolism 90 6609–6615.
- Skorupskaite K et al. 2014 Human Reproduction Update 20 485–500.
- Abbara A et al. 2013 Advances in Experimental Medicine & Biology 784 63–87.
- Sonigo C et al. 2012 Journal of Clinical Investigation 122 3791–3795.
- Millar RP et al. 2017 Journal of the Endocrine Society 1 1362–1371.
- Comninos AN et al. 2014 Human Reproduction Update 20 153–174.
- Comninos AN et al. 2016 Brain Structure & Function 221 2035–2047.
- Comninos AN et al. 2017 Journal of Clinical Investigation 127 709–719.
- Pineda R et al. 2017 Neuroendocrinology 104 223–238.
- Comninos AN & Dhillo WS 2018 Neuroendocrinology 106 195–202.
- Adekunbi DA et al. 2018 Journal of Neuroendocrinology 30 doi: 10.1111/jne.12572.
- Hellier V et al. 2018 Nature Communications 9 400.
- Mei H et al. 2013 Frontiers in Endocrinology 4 198.
- Jayasena CN et al. 2014 Journal of Clinical Investigation 124 3667–3677.
- Jayasena CN et al. 2014 Journal of Clinical Endocrinology & Metabolism 99 E953–E961.



{kind=link}
{kind=link}
{kind=link}