BACKGROUND
Gestational diabetes mellitus is defined as ‘hyperglycaemia first detected in the second or third trimester that is not clearly overt diabetes’.1 It is a common complication of pregnancy and is associated with increased risks to the mother and developing baby. For the former, this includes an increased risk of developing pre-eclampsia and later development of type 2 diabetes and for the latter, birth-related injuries, metabolic and physiological sequelae including fetal macrosomia, neonatal hypoglycaemia and in adolescence, insulin resistance and obesity.
The term ‘gestational diabetes’ was initially introduced to describe women with poor obstetric outcomes who had high glucose levels in subsequent pregnancies. Early diagnostic criteria were based on values that best predicted later development of maternal type 2 diabetes mellitus. Since then, understanding of the implications of developing hyperglycaemia in pregnancy has evolved considerably and diagnostic criteria are now based on the thresholds that best predict risk of adverse outcomes, in particular, fetal overgrowth.
EPIDEMIOLOGY
The historic absence of universally agreed screening strategies and diagnostic criteria has rendered it difficult to accurately establish the incidence of gestational diabetes. Furthermore, prevalence varies according to ethnicity and mirrors variations in prevalence of type 2 diabetes across the world. Rates are thought to be highest in the Middle Eastern and North African region with a median estimate of 12.9% (range 8.4–24.5%) of pregnancies affected by the condition and lowest in Europe, where the proportion of pregnancies affected is estimated at 5.8% (range 1.8–22.3%).2
PATHOPHYSIOLOGY
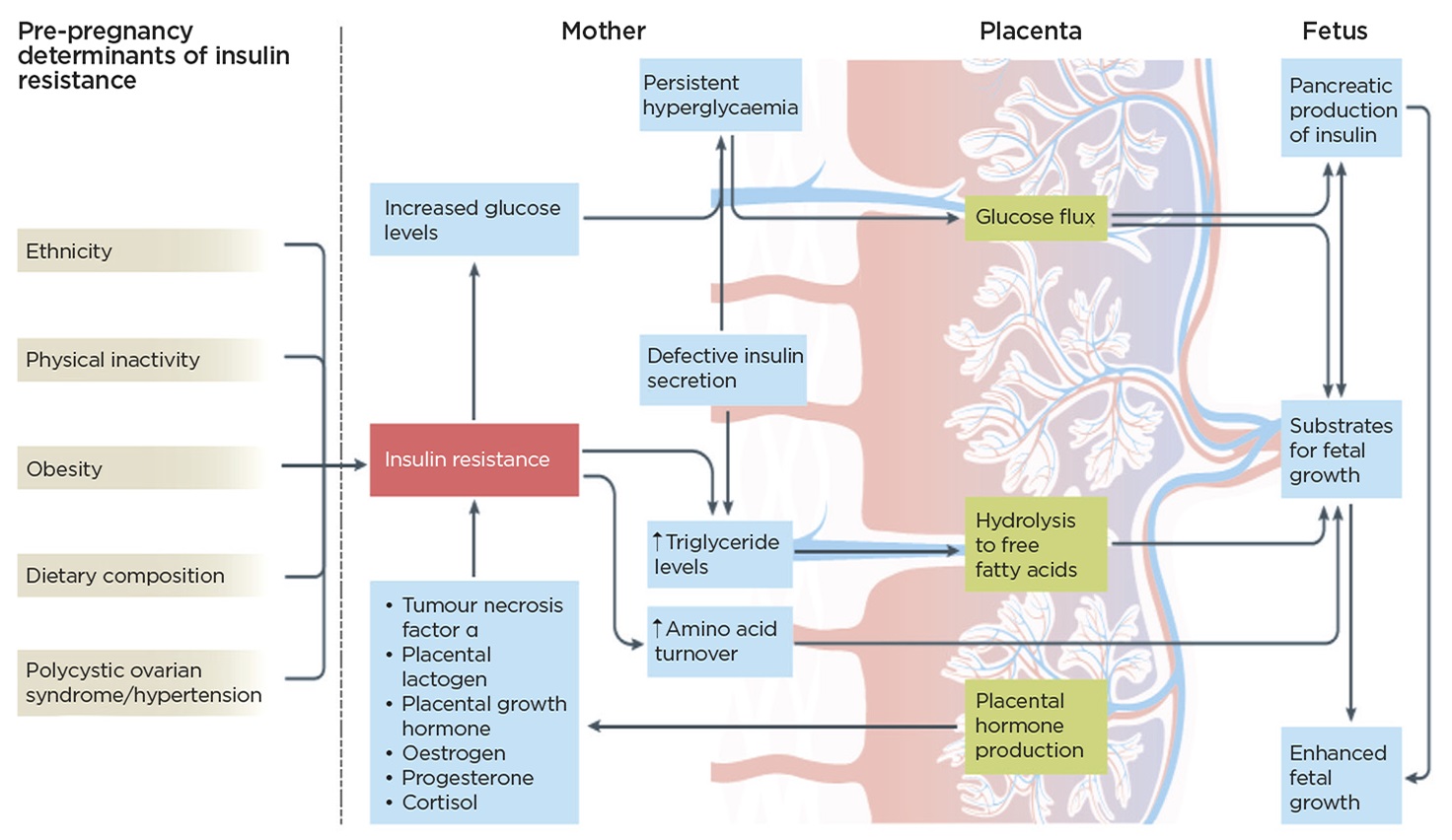
Pregnancy is characterised by an insulin resistance that increases with advancing gestation. The feto-placental unit is primarily responsible for driving this and, while the mechanisms are not fully understood, placental production of tumour necrosis factor α, placental lactogen, growth hormone, and increased cortisol and progesterone levels are all thought to contribute (Figure). To maintain maternal normoglycaemia, β-cell production of insulin increases. The resultant changes in maternal carbohydrate and lipid metabolism ensure the continuous and adequate delivery of substrate required for fetal development.

Factors contributing to maternal resistance and fetal growth. Reprinted by permission from Springer, Nature Reviews Endocrinology 12(9) Gestational diabetes mellitus: does an effective prevention strategy exist? Rochan Agha-Jaffar, Nick Oliver, Desmond Johnston, Stephen Robinson @Springer Nature 2016
Women unable to adapt to these pregnancy-induced physiological changes develop gestational diabetes. A significant overlap exists in the pathophysiology of gestational diabetes and type 2 diabetes, such that gestational diabetes could be seen to reflect an early stage of type 2 diabetes expressed under the conditions of pregnancy. Consistent with this is the observed increased rate of progression to type 2 diabetes in those with a history of gestational diabetes, with one meta-analysis demonstrating a cumulative incidence of type 2 diabetes ranging from 2.6% to over 70% in women who were assessed between 6 weeks and 28 years postpartum.3
THE CLINICAL PROBLEM AND PREVENTION STRATEGIES
The incidence of gestational diabetes and its complications are increasing, reflecting changing pre-gravid female demographics. Gestational diabetes is associated with a significant economic burden, with one model indicating a 34% increase in the cost of care for a woman whose pregnancy is complicated by hyperglycaemia.4 Although treatment has consistently been shown to reduce this, it nonetheless remains substantial. Furthermore, long term follow-up of infants born to mothers whose pregnancies are complicated by hyperglycaemia suggests that adiposity remains a significant problem despite effective treatment and management.5
Therefore, preventing pathological hyperglycaemia during pregnancy has several theoretical benefits: reduction in associated immediate maternal and fetal adverse outcomes, potential for improvements in the risk of long term sequelae and reductions in the economic burden to healthcare systems worldwide.
The randomised control trials investigating the impact of lifestyle interventions in preventing gestational diabetes have yielded conflicting results. This, in part, relates to the large degree of heterogeneity across the trials both in terms of the recruited cohort baseline demographics and the screening strategies and diagnostic criteria used to define the condition. However, despite the absence of identifying a clear preventive strategy, important signals from these trials have emerged, such as the benefits of interventions in improving pre-defined materno-fetal outcomes, for example fetal macrosomia, even in the absence of preventing maternal hyperglycaemia.6
‘Gestational diabetes is associated with a significant economic burden, with one model indicating a 34% increase in the cost of care for a woman whose pregnancy is complicated by hyperglycaemia.’
The benefits of dietary supplements in preventing gestational diabetes have also been explored. Fish oil supplementation failed to prevent gestational diabetes, but probiotics have been shown to benefit women at very high risk. While preliminary data in open label trials demonstrated a potential positive impact of supplementation with myo-inositol, this was not replicated in a double blind randomised trial of myo-inositol versus placebo.7 Finally, randomised controlled trials investigating the role of metformin in obese pregnant women have not shown benefits in preventing gestational diabetes, although metformin was associated with a reduced incidence of pre-eclampsia in one trial.8,9
With the increase in incidence of gestational diabetes being observed worldwide and the associated long-term complications, including that of the insulin resistance and obesity demonstrated in young adolescents exposed to in utero hyperglycaemia, research should continue to identify preventative strategies that can be easily implemented, particularly during the preconception period.
Rochan Agha-Jaffar, Consultant, Imperial College Healthcare NHS Trust
REFERENCES
- WHO Guideline Development Group 2013 Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. www.who.int/diabetes/publications/Hyperglycaemia_In_Pregnancy/en/.
- Zhu Y & Zhang C 2016 Current Diabetes Reports 16 7.
- Bellamy L et al. 2009 The Lancet 373 1773–1779.
- Gillespie P et al. 2013 Diabetes Care 36 1111–1116.
- Landon MB et al. 2015 Diabetes Care 38 445–452.
- Agha-Jaffar R et al. 2016 Nat Rev Endocrinol 12 533–546.
- Farren M et al. 2017 Diabetes Care 40 759–763.
- Chiswick C et al. 2015 The Lancet Diabetes & Endocrinology 3 778–786.
- Syngelaki A et al. 2016 New England Journal of Medicine 374 434–443.



{kind=link}