
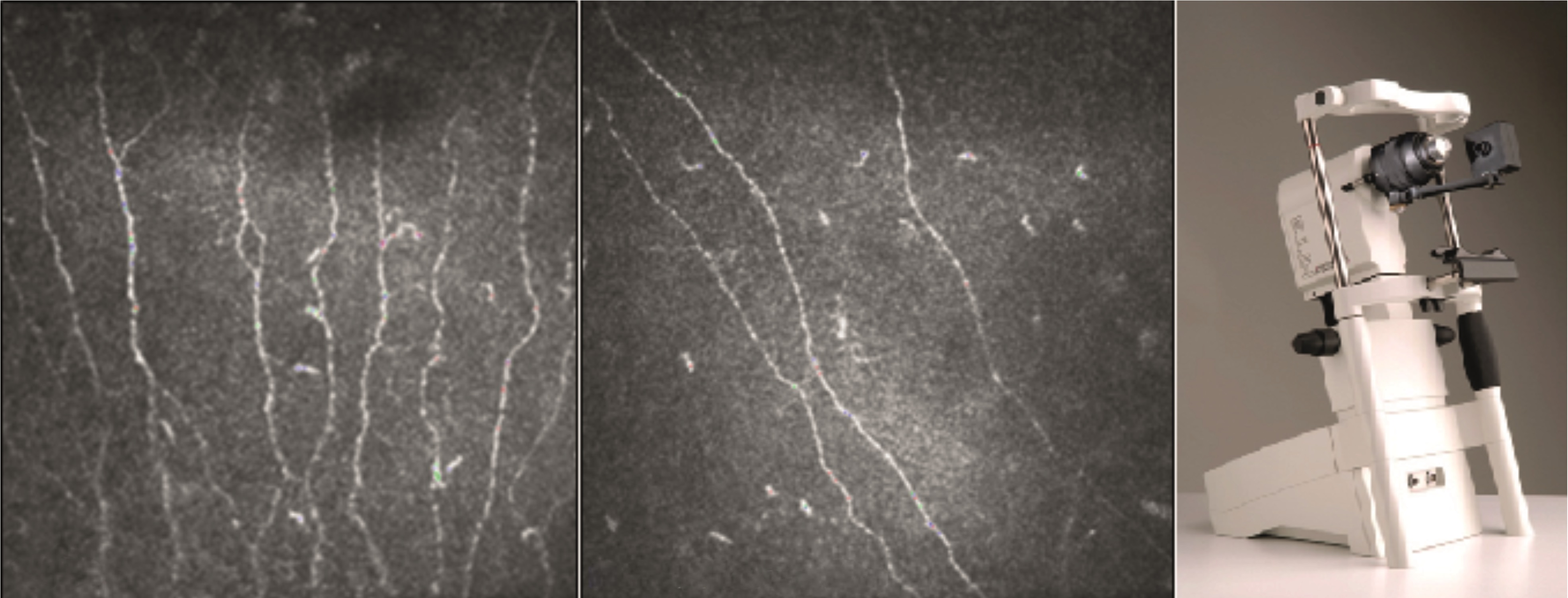
Figure 1. Corneal confocal microscopy in healthy normoglycaemic volunteer (left panel) and in an individual with established diabetic neuropathy (middle panel). A Heidelburg HRT3 corneal confocal microscope with corneal module (right panel). ©Sanjeev Sharma, Ipswich Hospital
The convergence of two unique, individually devastating complications – diabetic neuropathy (DN) and peripheral vascular disease – in addition to abnormal local host immune responses, a tendency to develop infections and the impact of ambulatory biomechanics in the foot makes diabetic foot disease (DFD) one of the most complex conditions to manage.
Coupled with a lifetime incidence risk of 19‒35% for the development of DFD and a 3-year recurrence rate of 60%, individuals with DFD are at high risk for amputation. Mortality is also unusually high in those with DFD; recent estimates suggest a rate in excess of 50% over 5 years, higher than many common cancers.
The modern management of a diabetic foot encompasses the early recognition and treatment of ischaemia, high quality wound care, prompt treatment of infection, off-loading and the correction of any underlying biomechanical anomalies, provided in a multidisciplinary setting.1 Alongside this, most individuals with DFD will require a spectrum of supportive medical and psychological care.
DIABETIC NEUROPATHY
The development of DN (sensory, autonomic and, in later stages, motor), in particular the distal symmetrical phenotype, is perhaps the most important predisposing factor for diabetic foot ulceration (DFU). DN may also lead to neuropathic pain and development of Charcot neuroarthropathy.
While the precise sequence of neuropathic damage is unclear, recent studies have suggested that the small nerve fibres (Aδ and C fibres) which mediate pain, temperature and autonomic functions are perhaps the earliest to be involved, even prior to the development of large fibre changes.2 This recognition has been made possible due to the development of modern neuropathy assessment techniques.
Corneal confocal microscopy (Figure 1) can accurately quantify corneal innervation in the human sub-basal plexus. It has been shown that reductions in corneal innervation occur early in the course of type 2 diabetes and worsen with increasing severity of DN, and that such changes run parallel to decrements in intraepidermal nerve fibre density at the distal leg.3
The laser Doppler flare technique (LDIfl are) is another emerging sensitive technique to assess small nerve fibre function which, in addition to picking up early small fibre abnormalities, is able to demonstrate improvements in neural function, for example after correction of hypothyroidism.4
Sudoscan® can quantitatively assess sudomotor function, a marker of cutaneous autonomic neuropathy, in a clinic setting. The novel Vagus™ device allows for bedside assessment of cardiovascular autonomic neuropathy, once the domain of the neurophysiology lab. Sadly, despite extensive research, apart from good glucose control, there are no licensed disease-modifying agents for DN.
PERIPHERAL ARTERIAL DISEASE (PAD)

Figure 2. Left pedal artery loop angioplasty in a patient with second toe osteomyelitis. ©KingsDFC
Peripheral obliterative arteriopathy is present in 50–60% of patients with DFU. This is classically distal and bilateral, involving most commonly the below knee and pedal vessels. It has been an area of significant advance – current technology allows for better characterisation of the PAD and there have been significant advances in both endovascular and surgical techniques of revascularisation.5 Transcutaneous oxygen measurements and laser Doppler perfusion assessment allow for objective assessment of the functional impact of any vascular insufficiency and may predict healing or the risk of amputation.
One important development has been the ability of modern percutaneous endovascular techniques to summarily revascularise the distal crural, pedal and, if necessary, even the digital vessels (Figure 2). When used effectively with a high quality foot service, remarkable outcomes have been reported.6 Even the traditional surgical approach has evolved, thanks to new techniques of ultra-distal bypass and hybrid procedures, whereby, in the latter, both a surgical bypass and endovascular revascularisation are undertaken concurrently.5 It is crucial as part of the medical management to evaluate the conditions of the other vascular regions such as the coronary and carotid arteries.
INFECTION: DIAGNOSIS AND MANAGEMENT
Infection frequently complicates DFU, increasing the risk of amputation. While the index infection in western Europe is classically caused by gram-positive cocci, in particular Staphylococcus aureus, the milieu in chronic DFU is often polymicrobial. How we evaluate the presence of infection is crucial.

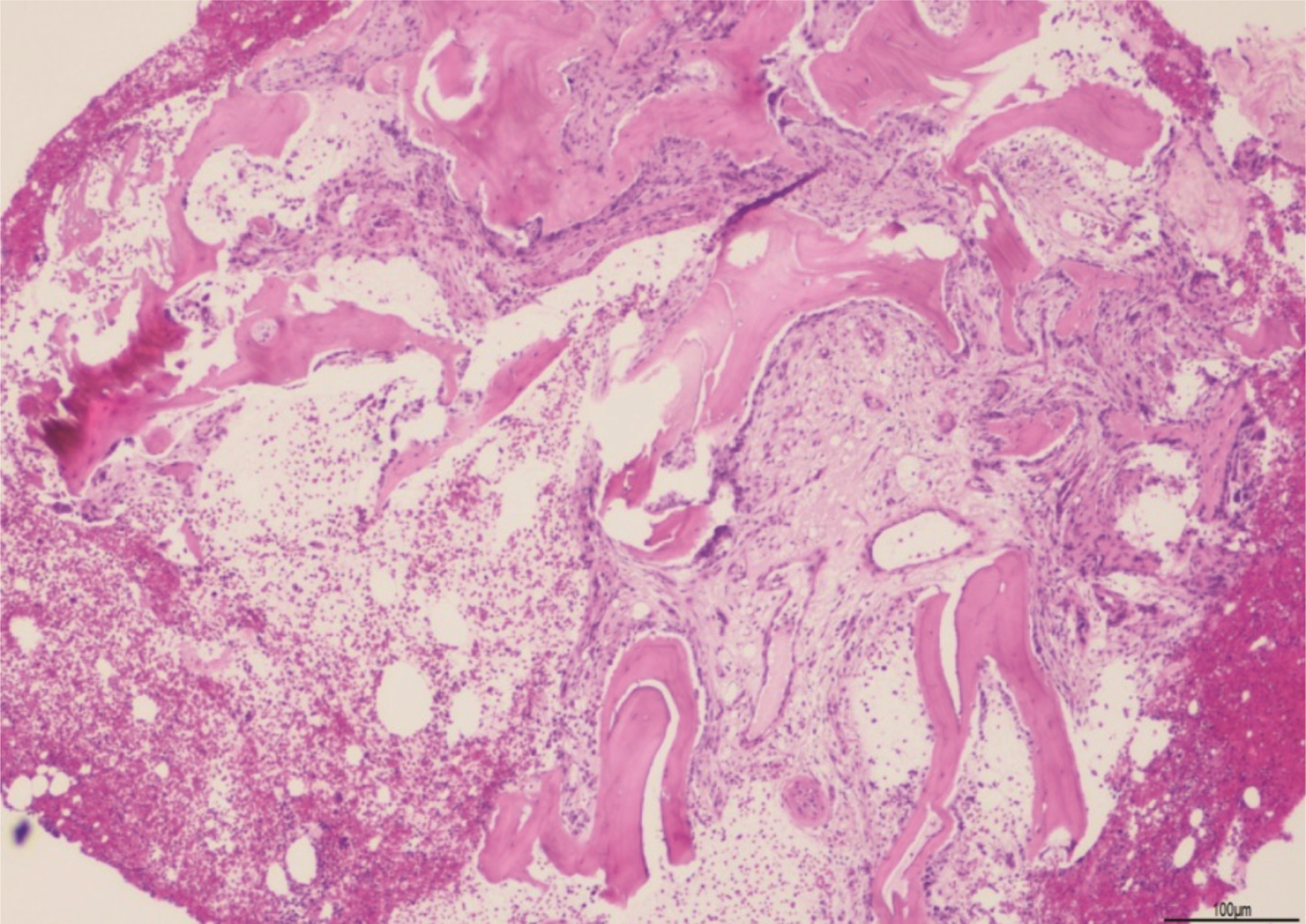
Figure 3. Bone biopsy showing core of cancellous bone trabeculae forming a mixture of viable bone and new reactive woven bone. There is a patchy infiltrate of neutrophils and plasma cells. The features are of subacute bacterial osteomyelitis. ©Dr John Salisbury, King’s College Hospital
The recently published CODIFI (Concordance in Diabetic Foot Ulcer Infection) study reported that 58% of pathogens differed between wound swab and tissue specimens.7 Pathogens (as compared to non-pathogens) were more frequently identified in tissue specimens, with the additional observation that clinicians were more inclined to make changes to antibiotic therapy based on tissue specimen results. 16S rRNA quantitative polymerase chain reaction (qPCR) and metagenomic sequencing techniques are being increasingly deployed to determine specimen biodiversity, allowing faster and arguably more reliable identification of culture-hardy bacteria.8
For the diagnosis of diabetic foot osteomyelitis (DFO), in addition to the traditionally utilised probe-to-bone test (a clinical indicator) and plain radiography, hybrid imaging techniques such as 99mTc WBC-SPECT/CT (99mTc-white blood cell single-photon emission computed tomography/ computed tomography) and [18F]FDG-PET ([18F]fluorodeoxyglucose-positron emission tomography) have been validated to evaluate the location and extent, and to distinguish bone from soft tissue infections.9 However, the gold standard for the diagnosis of DFO is a bone biopsy (surgical or percutaneous) which provides histological evidence (acute and/or chronic inflammatory cells, necrosis) alongside microbiological information to target antimicrobial therapy (Figure 3). In forefoot predominant DFO with viable bone, remission may be achieved with antibiotics and podiatric wound care only.
CHARCOT NEUROARTHROPATHY (CN)

Figure 4. Left foot hind-foot and mid-foot reconstruction (right panel) for severe Charcot deformity (left panel). L, left; W/T, weight. ©KingsDFC
Injury to the diabetic neuropathic foot can trigger inflammation and aggressive osteolysis resulting in multiple fractures and bone fragmentations. Ongoing research has focused on understanding the pathogenic mechanisms driving such activity, such as the osteoclastogenic cytokine receptor activator of nuclear factor-κβ ligand RANKL, and on exploring the role of proinflammatory cytokines such as tumour necrosis factor-α. This raises the potential of future putative pharmacologic therapeutic options, something we lack currently. Contemporary orthopaedic reconstruction techniques offer a new hope to those with gross deformities and facing amputation (Figure 4).
WOUND CARE AND OTHER DEVELOPMENTS
We have not discussed the contemporary thoughts on high quality wound care (which cannot be over-emphasised) and dressing choice (no dressing is singularly advantageous) in DFU prevention and, importantly, the emerging focus on tackling the variation in clinical outcomes within and between healthcare systems.
For interested colleagues, the NICE NG19 guideline provides an overview of frontline DFD care in the UK.10 The International Working Group on the Diabetic Foot (IWGDF; www.iwgdf.org) produces consensus guidelines every 4 years on the management and prevention of the diabetic foot and is another useful resource.
Perhaps the one biggest development is the recognition that the diabetic foot is a multi-system, cross-specialty disorder. It is developing into a sub-specialty in its own right, providing its practitioners with a stimulating balance between clinical practice and fast-moving research.
Erika Vainieri, ST3 in Diabetes and Endocrinology, North-West Thames Rotation, and Honorary Clinical Fellow, Diabetic Foot Clinic, King’s College Hospital, London
Prash Vas, Consultant in Diabetic Foot Medicine, King’s College Hospital, London
REFERENCES
- Vas PRJ et al. 2018 International Journal of Lower Extremity Wounds 17 7–13.
- Breiner A et al. 2014 Diabetes Care 37 1418–1424.
- Tavakoli M et al. 2010 Diabetes Care 33 1792–1797.
- Sharma S et al. 2018 Journal of Clinical Endocrinology & Metabolism doi:10.1210/jc.2018-00671.
- Huang DY et al. 2014 Seminars in Interventional Radiology 31 307–312.
- Uccioli L et al. 2010 Diabetes Care 33 977–982.
- Nelson A et al. 2018 BMJ Open 8 e019437.
- Spichler A et al. 2015 BMC Medicine 13 2.
- Lauri C et al. 2017 Diabetes Care 40 1111–1120.
- NICE 2016 Diabetic Foot Problems: Prevention and Management www.nice.org.uk/guidance/NG19.




{kind=link}
{kind=link}
{kind=link}
{kind=link}