Our patients have high expectations of what vitamin D supplements can achieve, but often express concerns about the safety of calcium tablets. We now have the advantage of several large new vitamin D trials, albeit with much less happening on the calcium front, yet the importance of calcium co-administration remains a dark horse here.
These trials continue to raise doubts as to what can be achieved by raising serum levels in populations that are already largely vitamin D-replete: i.e. with serum levels 50nmol/l or above, as proposed by the US Institute of Medicine.1 Other thresholds have been proposed by other professional bodies, but with less persuasive arguments. The definition was based on skeletal outcomes, since there continues to be a lack of positive intervention studies for other outcomes (as we shall see below).
As endocrinologists, we also have to consider any realistic non-calciotropic effects of vitamin D, such as potential effects on thyroid autoimmunity, polycystic ovary syndrome, development of diabetes (including gestational diabetes; GDM), obesity, and the progression and complications of other endocrine disorders.
'As endocrinologists, we have to consider any realistic non-calciotropic effects of vitamin D, such as potential effects on thyroid autoimmunity, polycystic ovary syndrome, development of diabetes, obesity, and the progression and complications of other endocrine disorders.'
CALCIUM
In the anti-resorptive treatment area, some of the bisphosphonates have been evaluated without calcium supplementation, and the results have been good.2 Thus, in patients on a dairy-rich Western diet who do not suffer from malabsorption or hypoparathyroidism, we may not need to rigorously enforce calcium supplements, though they have been co-administered in the majority of the original randomised controlled trails for osteoporosis drugs.
While avoiding calcium supplements in favour of dairy products seems intuitively right, there is no evidence that calcium supplements have a less favourable cardiovascular risk profile than dairy,3 and it is hard to understand why a phosphate-rich calcium source would be kinder to our vessels. However, calcium supplements can be followed by a transient spike in serum calcium, so repeating a serum calcium measurement in the fasting state, if initially raised in supplement users, saves time and work in the clinic.
VITAMIN D
There is genetic variability in the metabolism of vitamin D. This may require the occasional patient to require surprisingly high doses of vitamin D, especially initially, when fat stores are also being replenished. This aside, in the UK, the upper safe intake is considered to be 100µg (4000IU) daily, or ten times the 10µg (400IU) daily dose, which is the present supplementation in adults recommended by the Government.
COVID-19
The last few months have brought up the question of vitamin D in the prevention or treatment of COVID-19. In their 204-page rapid review, NICE and the Scientific Advisory Committee on Nutrition do not endorse vitamin D supplementation specifically to prevent or treat COVID-19, except as part of a clinical trial. Trials are in progress. The panel considered studies with primary outcomes being mortality, intensive care unit admission or hospitalisation. The panel also considered reviews of existing literature regarding vitamin D in preventing acute respiratory infections. Here, no protection was demonstrated in adults or when using vitamin D doses higher than 1000IU (25µg) per day.

Recent evidence on vitamin D supplementation has been disappointing in the cardiovascular, endocrine and musculoskeletal fields, but has shown a potential positive signal in the cancer area. Credit: Bo Abrahamsen
OTHER FIELDS
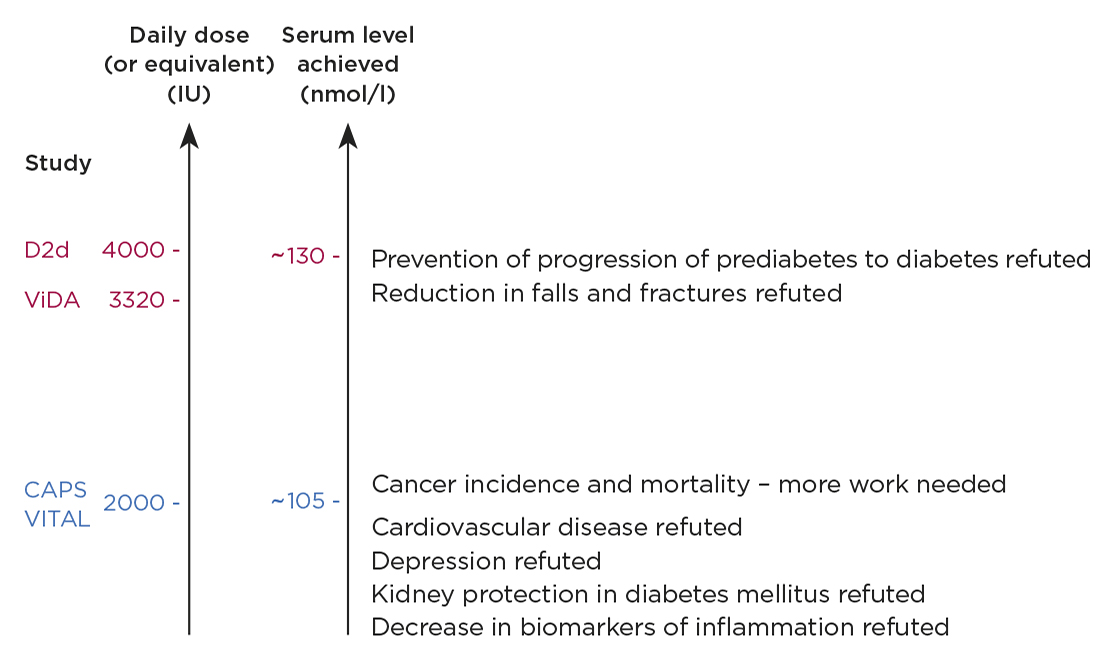
New evidence on vitamin D supplementation published in the last year or two has been fundamentally disappointing in the cardiovascular, endocrine and musculoskeletal fields, but has shown a potential positive signal in the cancer area (see Figure).
Large controlled vitamin D trials of 2000–4000IU daily (or equivalent but intermittent doses), capable of raising mean 25-hydroxyvitamin D (25-OHD) levels to above 100nmol/l, failed to reduce falls or fractures, failed to prevent cardiovascular disease, depression, progression from prediabetes to diabetes, and failed to offer kidney protection in diabetes or to decrease biomarkers of inflammation. Short term trials of the impact of vitamin D on lipid status have shown no effect or even a worsening.
Though the risk of GDM has been reported as being higher with vitamin deficiency, this may be due to confounding factors. It remains unclear whether vitamin D supplementation improves maternal or newborn outcomes in GDM, though smaller studies have been supportive, as recently reviewed elsewhere.4 The role of vitamin D deficiency in the development and prognosis of autoimmune thyroid disease is similarly controversial and interesting, but does not at present justify the use of vitamin D supplements in prevention or treatment of thyroid autoimmunity.5
The cancer findings are highly puzzling. The CAPS and VITAL trials both pursued cancer incidence as a primary outcome and the vitamin D dose used was 2000IU daily in both studies, over durations of 4 and 5.3 years respectively. Does calcium matter? The combination of calcium and vitamin D used in the CAPS trial resulted in a near-significant reduction in all-type cancer (hazard ratio (HR) 0.70, 95% CI 0.47–1.02, P=0.06), with significant findings in post-hoc analyses,6 while there was no signal at all in the VITAL study (HR 0.96, P=0.47).7 A recent meta-analysis supports an effect of vitamin D supplements on cancer mortality (five trials, RR 0.87 (95% CI, 0.79–0.96)), though no effect on cancer incidence.8
IN CONCLUSION
The role of vitamin D supplements in endocrine practice remains controversial, with new, large, randomised controlled trials failing to provide compelling evidence that even moderately high vitamin D doses, approaching the official upper safe limit of 4000IU (100µg) per day, lead to improved endocrine or metabolic outcomes in the general population. Intriguingly, cancer results looked more promising, where calcium was co-administered.
By nature, vitamin D is a threshold nutrient, and it appears increasingly unlikely that one size fits all, irrespective of baseline status. Thus, there could be vitamin D-deficient patient groups who benefit in terms of outcomes that were not significantly improved in the general, more replete, population. At present, the cancer arena offers more promise than the metabolic, endocrine or cardiovascular field as far as upper level doses of vitamin D in the general population are concerned.
BO ABRAHAMSEN
Professor, Consultant Endocrinologist, Department of Clinical Research, University of Southern Denmark, Holbæk Hospital, Denmark
REFERENCES
A more complete list is available from the author at [email protected].
- Rosen CJ et al. 2012 Journal of Clinical Endocrinology & Metabolism 97 1146–1152.
- Reid I et al. 2018 Calcified Tissue International 93 P068.
- Michaelsson K et al. 2014 BMJ 349 g6015.
- Rodrigues MRK et al. 2019 PLoS One 14 1–16.
- Vieira IH et al. 2020 Nutrients 12 1–20.
- Lappe J et al. 2017 JAMA 317 1234–1243.
- Manson JAE et al. 2020 Journal of Steroid Biochemistry & Molecular Biology 198 105522.
- Keum N et al. 2019 Annals of Oncology 30 733–743.



{kind=link}