It is 99 years since Leonard Thompson was given an injection of bovine insulin. In the intervening decades, we have developed effective replacement therapy for the majority of the classical hormone deficiencies. With the advent of recombinant human parathyroid hormone (rhPTH(1−84); ‘Natpar’ in Europe or ‘Natpara’ in North America), we can finally complete the set.
VITAMIN D SUPPLEMENTATION
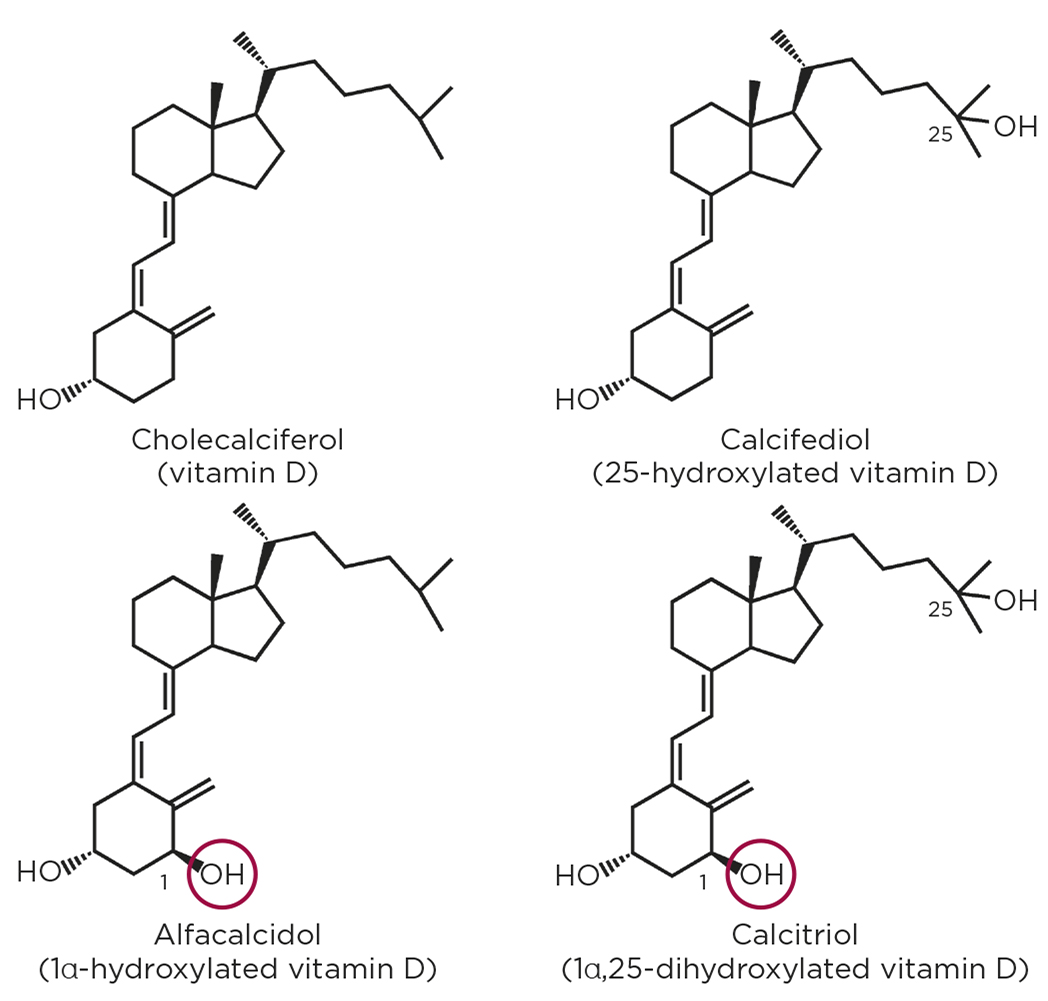
Conventionally, hypoparathyroidism has been treated by ‘bypassing’ the missing hormone and administering a pharmacologic mimic of one of its key downstream mediators. This takes the form of activated vitamin D as 1α-hydroxylated vitamin D (alfacalcidol) or 1α,25-dihydroxylated vitamin D (calcitriol), and is given with supplemental calcium.

Figure 1. Molecular structure of 'plain' vitamin D, calcifediol (25-hydroxylated vitamin D), alfacalcidiol (1α-hydroxylated vitamin D) and calcitriol (1α,25-dihydroxylated vitamin D), highlighting the 1α-hydroxyl group.
The hydroxyl group in the 1α position (see Figure 1) is the crucial molecular feature in activating vitamin D and enabling it to bind to the vitamin D receptor (VDR) and activate downstream signalling. One role of PTH is to regulate the hydroxylation of vitamin D at this location, to effect activation (Figure 2). Since PTH is a peptide hormone which is normally poorly active or completely inactive via the oral route, administration currently must be via a parenteral route. Few people like injecting themselves and, historically, the alternative (1α-hydroxylated vitamin D metabolites with or without calcium) that is orally bioavailable has assumed primacy.
ASSOCIATED DRAWBACKS
However, there are numerous and significant drawbacks to the treatment of hypoparathyroidism with activated vitamin D and calcium. These include:
- a slow onset of action
- a prolonged duration of action
- difficulties with accurately titrating the dose and, most fundamentally,
- as this is not actual hormone replacement therapy, the missing hormone’s actions are not all accurately reproduced.
While PTH reduces tubular calcium excretion, alfacalcidol and calcitriol (especially in combination with oral calcium salts) are associated with hypercalciuria, causing significant risk of nephrocalcinosis, nephrolithiasis and renal failure.1,2 Difficulties with titrating the dose of activated vitamin D compounds, combined with a perception that these are ‘only’ a vitamin (and by implication must be harmless), mean that many patients treated with these compounds have received less specialist attention3 and less intensive medical supervision and biochemical monitoring than required. This, in turn, is associated with a significant incidence of severe iatrogenic hypercalcaemia and demonstrable patient harm, leading the former National Patient Safety Agency to issue a safety alert about alfacalcidol.4 In addition to all these considerations (and arguably, most importantly of all), many with hypoparathyroidism treated with activated vitamin D-based regimens experience poor quality of life and frequent unplanned hospital attendances for hypo- and hypercalcaemia.3
There is, therefore, a very real and clear need for improved treatments for hypoparathyroidism.

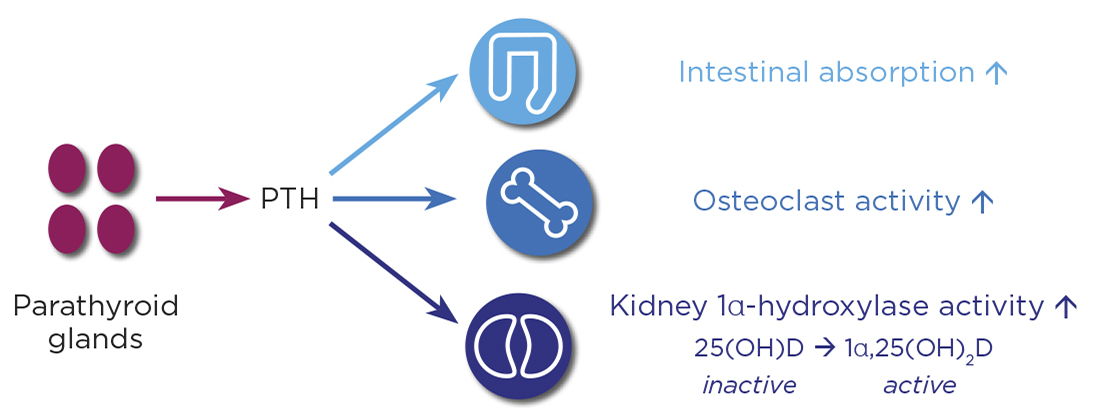
Figure 2. PTH secreted from the parathyroid glands stimulates 1α-hydroxylase in the kidneys to activate 25-hydroxylated vitamin D to 1α,25-dihydroxylated vitamin D.
RECOMBINANT HUMAN PTH
What could be better than actual hormone replacement therapy? Recombinant PTH(1−84) is now licensed as a treatment for hypoparathyroidism in Europe, North America and other regions, but how did we get here, and what are the ongoing challenges yet to be resolved with this treatment?
rhPTH(1−34), originally teriparatide, now biosimilars such as Movymia, is licensed for the treatment of osteoporosis. However, long before its licensing for osteoporosis, attempts were made to augment treatment of hypoparathyroidism with subcutaneous teriparatide injections and, later, subcutaneous teriparatide infusion therapy. The earliest report dates back to 1986.5 Initial experience was encouraging, including (importantly) reductions in urinary calcium excretion. Many reports have confirmed these favourable outcomes.6,7
In 2013, the results of the first large randomised controlled trial (RCT) of full length rhPTH(1−84) for treatment of hypoparathyroidism (REPLACE) were published.8 Since then, results of other RCTs have been published,9−11 by and large confirming the favourable safety and efficacy profile of rhPTH(1−84) as a treatment for hypoparathyroidism.
Favourable effects include reduced calciuresis, improved quality of life, reduced activated vitamin D and oral calcium supplementation dose requirements and improved bone turnover marker profiles. These suggest that, in the long term, there may also be favourable effects on fracture risk and other aspects of skeletal health from PTH replacement therapy. High rates of attainment of normal albumin-adjusted serum calcium levels are also seen in such RCTs.
'Favourable effects include reduced calciuresis, improved quality of life, reduced activated vitamin D and oral calcium supplementation dose requirements and improved bone turnover marker profiles.'
There is a theoretical concern about osteosarcoma, but this signal is derived from rodent data. In nearly 15 years of post-licensing/‘real world’ use of teriparatide, where the same concern pertains, there has been no significant confirmation of this signal in human clinical use. In excess of 5 years’ trial data for rhPTH(1−84) are now available. Thus far, they are very reassuring.
Typical rhPTH(1−84) doses range between 25 and 100µg, given as a once daily subcutaneous injection. They are usually given in combination with oral calcium supplements and activated vitamin D, although some individuals can achieve normocalcaemia without oral supplements.
Development of an oral preparation of PTH(1−34) is also underway, where gastric degradation of the peptide is prevented by a combination of chemical/physical protection. This has entered preliminary trials in hypoparathyroidism which have resulted in promising results. This development may help overcome the fear of self-injection of PTH.
IN CONCLUSION
Nearly 100 years after the dawn of the hormone replacement era, endocrinologists are finally seeing the availability of hormone replacement therapy for hypoparathyroidism. This is only the beginning, and many unanswered questions remain about the optimal use of this treatment. The field is still evolving, and many patients are likely to remain on conventional activated vitamin D plus oral calcium supplementation therapy for some time.
Even for those lucky enough to have the option of rhPTH(1−84) therapy, it should probably mainly be seen as an adjunct for now, to be used alongside activated vitamin D and oral calcium supplements. There is certainly more work to be done!
DAVID BAWDEN
Specialist Registrar in Endocrinology, Norfolk and Norwich University Hospital
WILLIAM D FRASER
Professor of Medicine and Dean of Medical School, University of East Anglia
JEREMY TURNER
Consultant Endocrinologist and Honorary Professor, Norfolk and Norwich University Hospital and Norwich Medical School
REFERENCES
- Bilezikian JP et al. 2016 Journal of Clinical Endocrinology & Metabolism 101 2313–2324.
- Bollerslev J et al. 2015 European Journal of Endocrinology 173 G1−G20.
- Parathyroid UK 2017 Living with Hypoparathyroidism www.parathyroiduk.org/wp-content/uploads/2018/05/Living-with-chronic-hypoparathyroidism-final-report.pdf.
- NHS 2011 NPSA Signal: Prevention of Harm with Alfacalcidol Preparations www.sps.nhs.uk/articles/npsa-signal-prevention-of-harm-with-alfacalcidol-preparations-sept-2011.
- Furlong TJ et al. 1986 Australian & New Zealand Journal of Medicine 16 794−798.
- Winer KK et al. 1998 Journal of Clinical Endocrinology & Metabolism 83 3480–3486.
- Winer KK et al. 1996 JAMA 276 631–636.
- Mannstadt M et al. 2013 Lancet Diabetes & Endocrinology 1 275−283.
- Bilezikian JP et al. 2017 Clinical Therapeutics 39 2096−2102.
- Lakatos P et al. 2016 Endocrine Practice 22 523−532.
- Mannstadt M et al. 2019 Journal of Clinical Endocrinology & Metabolism 104 5136–5147.


{kind=link}
{kind=link}