It is anticipated that 1 in 500 women of reproductive age will have a prolactinoma. Elevated prolactin levels inhibit the release of luteinising hormone and follicle-stimulating hormone. The degree of menstrual disturbance corresponds to the degree of hyperprolactinaemia. Even in the presence of regular cycles, hyperprolactinaemia is thought to make conditions less favourable for embryo implantation.
MEDICAL MANAGEMENT
‘Specialist nurses are often best placed to recognise the failure of medical treatment in a timely manner. There is also a key role to be played in counselling patients regarding alternative management options and advocating for the consideration of surgery, as and when appropriate.’
Dopaminergic agonists (DA) are the primary therapy for patients with prolactinomas. Medical therapy is remarkably effective in restoring gonadal function and fertility. Cabergoline is widely recognised to be superior to bromocriptine, both in terms of tolerability and efficacy.
DA should be continued in women seeking pregnancy. Observed rates of spontaneous miscarriage, preterm delivery and neonatal malformation are comparable in women taking DA to those in the general population. Current guidelines recommend the use of cabergoline at the lowest possible effective dose until a pregnancy is confirmed.
Common side-effects, such as nausea, postural hypotension and nasal stuffiness, can often be mitigated by gradual dose titration. However, there remains a significant group of patients in whom DA intolerance and/or resistance necessitate alternative treatment strategies.
Neuropsychiatric side-effects remain particularly challenging. The prevalence of impulse-control disorders in patients treated with DA has historically been underestimated, and is now recognised to be up to 1 in 6 patients.

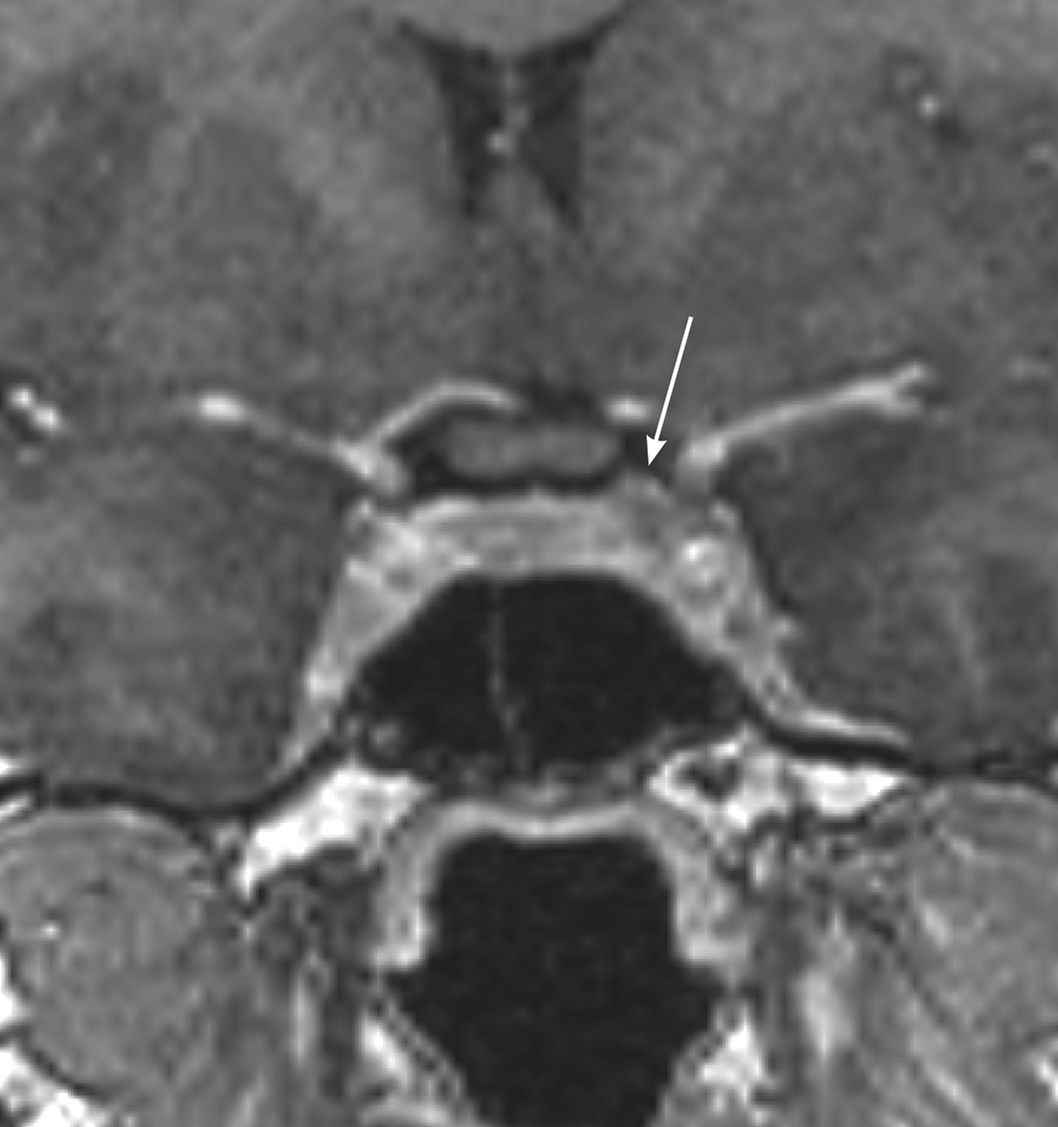
Figure. MRI with arrow showing left-sided microprolactinoma, which was removed at trans-sphenoidal surgery with positive histology and subsequent remission. ©Mark Gurnell, Addenbrooke’s Hospital
ALTERNATIVE TREATMENT STRATEGIES
Hormone replacement therapy can be used to ameliorate hypogonadism. However, it does not restore fertility.
Surgical intervention offers an alternative management option. Selective adenomectomy has been demonstrated to be both safe and effective in several neurosurgical cohorts. Importantly for this group of patients, anterior pituitary function is almost always preserved (100% of patients were eupituitary at three months in a recent series).
THE ROLE OF THE SPECIALIST NURSE
As a titrated therapy, management with DA requires regular blood testing and subsequent dose adjustment. This can be overseen by a specialist nurse with knowledge of this area of practice.
Additionally, patients starting on DA need clear counselling about the potential side-effects at the point of initiation. They also require a clear mechanism or ‘point of contact’ for reporting and discussing potential concerns once on treatment.
Specialist nurses are often best placed to recognise the failure of medical treatment for a prolactinoma in a timely manner. There is also a key role to be played in terms of counselling patients regarding alternative management options and advocating for the consideration of surgery, as and when appropriate.
AN ILLUSTRATIVE CASE
A woman in her late 30s presents with oligomenorrhoea and difficulty in conceiving. Hyperprolactinaemia is identified and non-tumoural causes are excluded. Pituitary magnetic resonance imaging (MRI) confirms a sub-centimetre adenoma. Cabergoline is initiated at 250µg twice a week; however, dizziness and nasal stuffiness are intolerable at higher doses. Bromocriptine and quinagolide produce a similar profile of adverse effects. Exploratory trans-sphenoidal surgery is discussed as a potential alternative. Selective adenomectomy is subsequently undertaken, with post-operative normalisation of prolactin levels.
Laura Serban
Pituitary Specialist Nurse, Wolfson Diabetes and Endocrine Clinic, Institute of Metabolic Science, Cambridge University Hospitals NHS Foundation Trust, Addenbrooke’s Hospital, Cambridge



{kind=link}