In issue 142 of The Endocrinologist (Winter 2021), Kerri Devine and Rebecca Reynolds discussed how maternal usage of glucocorticoids during pregnancy can influence the baby’s ability to regulate glucocorticoids, which may affect their metabolism through life.
It may seem implausible that our lives are so influenced by how our mother’s body reacted to stresses, toxins, infections and so on during pregnancy, and how growth and development during our first few years of life could lead to disease in middle age. However, we are now beginning to understand the full extent of David Barker’s theory, proposed in 1993, on the developmental origins of health and disease. As we approach its 30th anniversary, it is useful to take stock of what we currently know, so we can build towards the future.1
THE PLACENTA: MATERNAL/FETAL INTERFACE
During the nine months of pregnancy, any interaction between mother and baby occurs at the placenta. The placenta is formed from the fertilised egg, along with the growing baby, and is attached to the uterus. It grows with the baby to eventually weigh an average of 650g, and is roughly the size of a normal dinner plate.2 It is a truly unique organ in the body, taking on several crucial roles to allow the baby to grow successfully, and having both fetal and maternal blood flowing through it at any one time.
‘If we influence mums-to-be now, we could begin to alter the frequency of cardiovascular and metabolic disease in the next two generations to come.’
This, however, poses a problem. As the placenta itself is half maternal and half paternal in origin, it is essentially foreign graft tissue, and so the placental cells in contact with the maternal blood supply must constantly prevent recognition by maternal immune cells, whilst allowing transport of the required substances. The layer of cells in contact with the maternal circulation are termed the syncytiotrophoblast. This barrier of syncytial epithelium allows for the active and specific transport of substances, keeping fetal and maternal nutrient compositions distinct throughout pregnancy.3
UNDERSTANDING PLACENTAL TRANSFER
Our knowledge of placental transfer is not robust at this time. We know gas exchange occurs, although our current understanding of the amount of exchange is limited in human pregnancy, being based on approximations through ex vivo work.4 We have strong evidence of 20 different amino acid transporters along the syncytial membrane, and that fatty acids can cross through, following a multi-stage progression with fatty acid-binding proteins, as well as active synthesis of cholesterol and steroids.5 Glucose transport proteins have been well categorised within the placenta, and we know that the expression of these proteins does change during pregnancy.6
The current mystery is the effect of the external factors that pregnant women constantly face. Any changes in the functioning of the placenta to limit the transfer of the above have the potential to severely limit the growth and development of the fetus. This, in turn, leads to long term changes in metabolism, and the development of diseases in later life, including cardiovascular and metabolic disorders.7

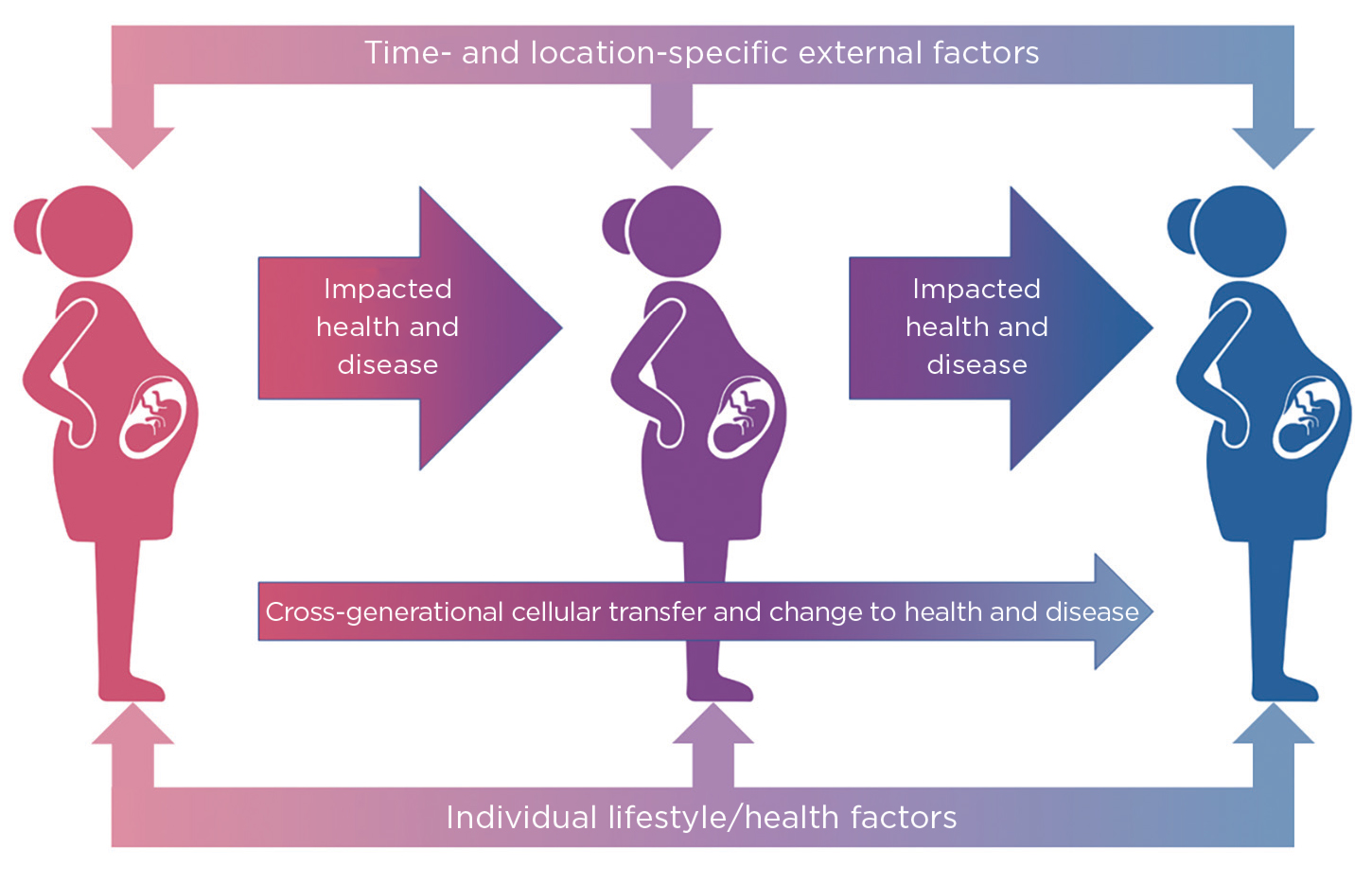
Figure. External factors such as environment, stress and employment, and lifestyle factors including diet and medications, can influence the health and development of a growing baby. These can impact lifetime health and disease. If they become pregnant, the same factors apply to this new growing fetus. However, the influence of the grandmother remains a considerable factor, through direct influence on the mother’s development and cross-generational transfer of cellular material. Created with BioRender.com
THE IMPACT OF EXTERNAL FACTORS
Some external factors are well documented (e.g. poor maternal diet, smoking during pregnancy and maternal stress), but there is a growing base of research which has shown that, during pregnancy, women may be exposed to over 50 different chemicals.8 Many of these are considered to be endocrine-disrupting chemicals, as exposure to them can alter normal physiological endocrine function, in part due to the high abundance of steroid hormone receptors present within the placenta. Large scale epidemiological studies have begun to make associations between these chemical exposures and adverse pregnancy outcomes.
A recent study has taken this one step further. Rzhetsky and collaborators have performed large scale statistical tests on country-wide health datasets, to investigate associations between external factors and the sex ratio at birth.9 Under normal circumstances, the proportion of boys at birth is usually slightly greater than 50%. This study found that the levels of chemicals found in pollution within a given area could potentially control the sex of a baby, although further analysis is required. If these chemicals and signals do have the power to decide fetal sex, there is no end to the possible changes that may occur during fetal growth and development.9
LIMITATIONS ON LAB WORK
Large epidemiological studies like that of Rzhetsky and colleagues are useful for adapting public health messages. However, without ‘wet lab’ approaches, the findings will always be associations, because our fundamental knowledge of what can and can’t cross the placenta is still lacking. This is where our understanding of the developmental origins of health and disease often comes to a halt. The clear ethical and practical issues surrounding the use of human placentas, hampered by a lack of consensus on procedural standardisation in isolating and purifying human placental tissue, have led researchers to routinely use litter-bearing rodents, which in itself presents wide-ranging challenges.
Ex vivo dual perfusion of the human placenta is a widely accepted method of understanding the pharmacological and physiological functions of the placenta, in particular regarding transfer from maternal to fetal circulations. This is achieved whilst maintaining both an approximate in vivo environment and an in vivo placental structure. Whilst the benefits to research are plain to see, this is a costly method of analysis in terms of both time and money, with a high preparation failure rate and the use of specialised equipment. Currently, only a handful of centres are even set up to do this type of placental work.4
Until we can systematically analyse both the transfer of substances across the human placenta and their interaction with maternal and fetal tissues, we may never know directly whether changes levels of hormones, chemicals, inflammatory markers and the like influence the health and disease of the next generation.
AN IMPACT ACROSS MANY GENERATIONS
We may, however, be setting our sights too short with Barker’s concept. A recent paper from Karlmark et al.10 has shown the presence of grandmaternal cells within cord blood samples. Due to the bidirectional exchange of cells during pregnancy, pregnant women have acquired maternal cells during their fetal life from their mother, which could transfer grandmaternal cells to their child through the maternal bloodstream during pregnancy. We have already seen transgenerational effects because of environmental exposures as, for example, children have an increased risk of asthma in the first six years of life if their grandmother smoked during early pregnancy, independent of maternal smoking.11
Whether this is a passive or active transfer is currently unknown, but it leads those researching the developmental origins of health and disease to begin to look further than the effect on health and disease in the next generation. If we influence mums-to-be now, we could begin to alter the frequency of cardiovascular and metabolic disease in the next two generations to come.
Gareth Nye
Lecturer of Anatomy and Physiology, University of Chester
REFERENCES
- Barker DJ et al. 1993 Lancet 341 938–941.
- Mayhew T et al. 2007 Placenta 28 233–238.
- Cleal J et al. 2011 Journal of Physiology 589 987–997.
- Nye GA et al. 2018 Journal of Physiology 596 5523–5534.
- Winterhager E & Gellhaus A 2017 Frontiers in Physiology doi:10.3389/fphys.2017.00951.
- Baumann MU et al. 2002 Endocrine 19 13–22.
- Hoffman DJ et al. 2021 Physiological Reviews 101 739–795.
- Gingrich J et al. 2020 Trends in Endocrinology & Metabolism 31 508–524.
- Long Y et al. 2021 PLoS Computational Biology doi:10.1371/journal.pcbi.1009586.
- Karlmark KR et al. 2021 EBioMedicine 74 103721.
- Lodge CJ et al. 2018 Clinical & Experimental Allergy 48 167–174.



{kind=link}