Klinefelter syndrome (KS) is a common aneuploidy in men, clinically characterised by small testes, gonadal failure (hypergonadotrophic hypogonadism), disrupted spermatogenesis (infertility), gynaecomastia and eunuchoid proportions (arm span exceeds height by ≥7cm).1,2 It affects 1 in 600 men, but 50−75% of men with KS go undiagnosed in their lifetime.1,3 Almost 90% of men with KS have an XXY karyotype, and the remaining 10% have mosaicism (46,XY/47,XXY), higher grade aneuploidy (48,XXXY/49,XXXXY), or structurally abnormal X chromosomes.1
'Effective management of patients with KS undergoing fertility treatment requires a multidisciplinary approach, including endocrinology, andrology, genetic counselling, psychology and nursing.'
The extent of mosaicism in KS causes an array of cognitive, psychosocial and physical symptoms which can affect men with varied degrees of severity. These include hypogonadism, gynaecomastia, tall stature, small phallus, reduced level of intelligence, depression, autism traits, schizotypal traits and social anxiety, which lead to impaired quality of life.1,4 Milder phenotype and lack of distinct dysmorphic features present a real challenge for early diagnosis.2
MANAGING KLINEFELTER SYNDROME
KS is characterised by primary testicular failure resulting in hypergonadotrophic hypogonadism with elevated luteinising hormone and follicle-stimulating hormone levels, and low testosterone. Testosterone replacement therapy is recommended for patients with KS once serum gonadotrophins begin to rise in early puberty, or when serum testosterone levels become hypogonadal.2,4,5 Infertility in men with KS ensues due to the progressive gonadal failure, where normal testicular architecture alters, causing tubular atrophy, sclerosis or maturation arrest, and ultimately degenerates to fibrosis and hyalinised tissue.
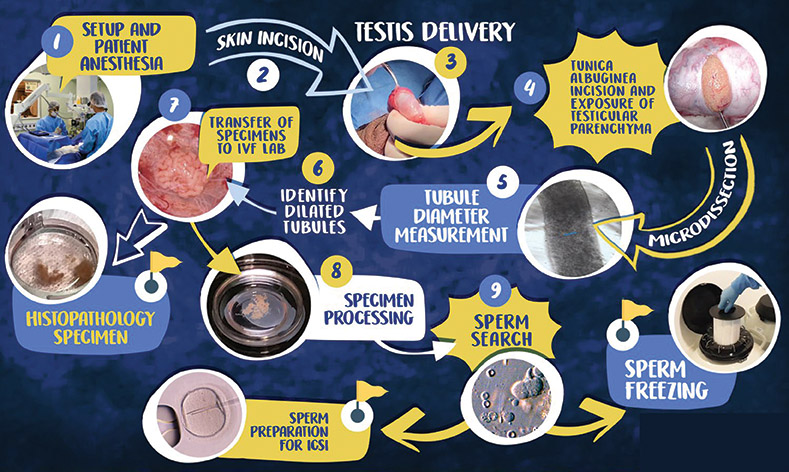
Advances in surgical techniques, in particular microsurgical testicular sperm extraction (micro-TESE), provides patients with KS with the possibility of fathering a child (Figure). A meta-analysis of 37 trials (n=1,248; mean age 30.9±5.6 years), showed that the surgical sperm retrieval rate per TESE cycle was achieved in almost half of the men with KS (44%; 95% CI 39–48%),7 although evidence on take-home baby rate after micro-TESE and female assisted reproductive treatment is still very limited.
Increasingly, the onset of puberty has been recognised as the critical time to address the fertility potential of men with KS, and early sperm retrieval and semen or testicular tissue cryopreservation has been recommended by several investigators, although there is still no robust evidence to support this.8 However, there is considerable controversy regarding this approach, given the ethical concerns surrounding non-essential invasive procedures in minors, as well as potential implications and confounding issues related to the adolescents’ and young adults’ comprehension and maturity to weigh risk–benefit.9 This needs to be considered on a case-by-case basis, and the patient with KS and their parent(s) should be adequately consulted and supported to make an informed decision.
For many adult patients, presentation with infertility while trying for a family leads to diagnosis of KS. A detailed semen analysis determines whether sperm collection may be feasible if healthy spermatozoa are present in the ejaculate. For patients with azoospermia, a pre-existing protocol for the management of this condition can be followed.10 This includes stopping testosterone replacement therapy, starting oral clomiphene citrate, and monitoring total testosterone and oestrogen levels throughout, followed by micro-TESE. Sperm can then be used for ‘synchronous sperm retrieval’, i.e. immediate use in combination with oocyte retrieval and/or cryopreserved for future use by the partner in her assisted fertility cycles with intracytoplasmic sperm injection. The former has higher success rates for positive pregnancy. However, the couple need to be consulted on the risk of not finding viable sperm during TESE, as oocyte retrieval can be an invasive and expensive procedure for the female partner.

The micro-TESE process. ©2021, Achermann APP et al., under exclusive licence to Springer Nature B.V.
THE NURSES’ ROLE IN SUPPORT
Effective management of patients with KS undergoing fertility treatment requires a multidisciplinary approach, including endocrinology, andrology, genetic counselling, psychology and nursing. Infertility can put couples under significant psychological, physical and financial stress, and the endocrine nurse plays a vital role in supporting patients with their treatment management and suggesting psychological referral as appropriate. Adopting a Nursing Process framework, the endocrine nurse provides a systematic approach to decision making and care planning, comprised of five stages: assessment, diagnosis, planning, implementation and evaluation.2 The patient and his partner should be actively involved in the decision-making process and consulted throughout the duration of the fertility treatment.
Assessment starts with a holistic evaluation of clinical, physiological and psychological needs, in order to highlight any current areas of negative impact. A medical history should also be taken from the patient’s partner, to identify any potential fertility issues and concerns. The endocrine nurse will support the couple to prepare for a potentially lengthy and stressful process, advise them accordingly and/or make appropriate referrals for counselling.
Once all assessments are completed, the treatment plan should be discussed and agreed with the multidisciplinary team. The endocrine nurse plays a crucial role in providing the patient with the relevant information about the fertility treatment changes and the TESE surgical procedure, including a detailed explanation of the success rates, based on available research and statistics from their local centre.
For successful implementation of the agreed care plan, the endocrine nurse needs to ensure that the patient understands the information provided regarding fertility treatment, and provides him with the opportunity to ask questions. Evaluation will be completed at designated time points, such as clinic appointments to monitor treatment progress and the patient’s overall physical and psychological well-being. The partner should also be involved in the follow up consultations and supported for assisted fertility treatment planning, when micro-TESE is successful in retrieving healthy sperm.
Brien Mehmet
PhD Candidate and Endocrine Nurse, School of Health Sciences, City University of London
Sofia Llahana
NIHR Post-doctoral Clinical Lecturer, Senior Lecturer in Advanced Clinical Practice and Consultant Nurse in Endocrinology, School of Health Sciences, City University of London, and Department of Diabetes and Endocrinology, University College Hospital, London
REFERENCES
- Gravholt CH et al. 2018 Endocrine Reviews 39 389–423.
- Dwyer AA & Quinton R 2019 In Advanced Practice in Endocrinology Nursing, Eds Llahana S et al., pp 853–870. Cham, Switzerland: Springer International Publishing.
- Bojesen A et al. 2003 Journal of Clinical Endocrinology & Metabolism 88 622–626.
- Jayasena CN et al. 2022 Clinical Endocrinology 96 200–219.
- Llahana S 2019 In Advanced Practice in Endocrinology Nursing, Eds Llahana S et al., pp 885–902. Cham, Switzerland: Springer International Publishing.
- Achermann APP et al. 2021 International Urology and Nephrology 53 2193–2210.
- Corona G et al. 2017 Human Reproduction Update 23 265–275.
- Mehta A & Paduch DA 2012 Fertility & Sterility 98 274–283.
- Dwyer AA et al. 2019 In Advanced Practice in Endocrinology Nursing, Eds Llahana S et al., pp 903–923. Cham, Switzerland: Springer International Publishing.
- Kailash Y et al. 2021 Frontiers in Reproductive Health doi:10.3389/frph.2021.636629.


{kind=link}