It is estimated that one in three women will experience abnormal uterine bleeding (AUB) at some point in their reproductive lives. Heavy menstrual bleeding is an unrecognised cause of iron deficiency anaemia, may require blood transfusion, and has a significant negative impact on emotional, social and material quality of life.1,2 Yet menstruation is taboo, meaning it is rarely discussed, under-researched and often suboptimally managed. A principal role of a specialist menstrual disorders service is to address the health inequalities that are all too often experienced by those who menstruate.
WHAT CONSTITUTES ‘TYPICAL’ AND ‘PROBLEMATIC’ MENSTRUATION?
Due to the embarrassment and shame that surrounds menstruation, many people do not know what typical menstrual bleeding comprises. This societal problem was previously compounded by a lack of standardised terminology in menstrual research and clinical practice.
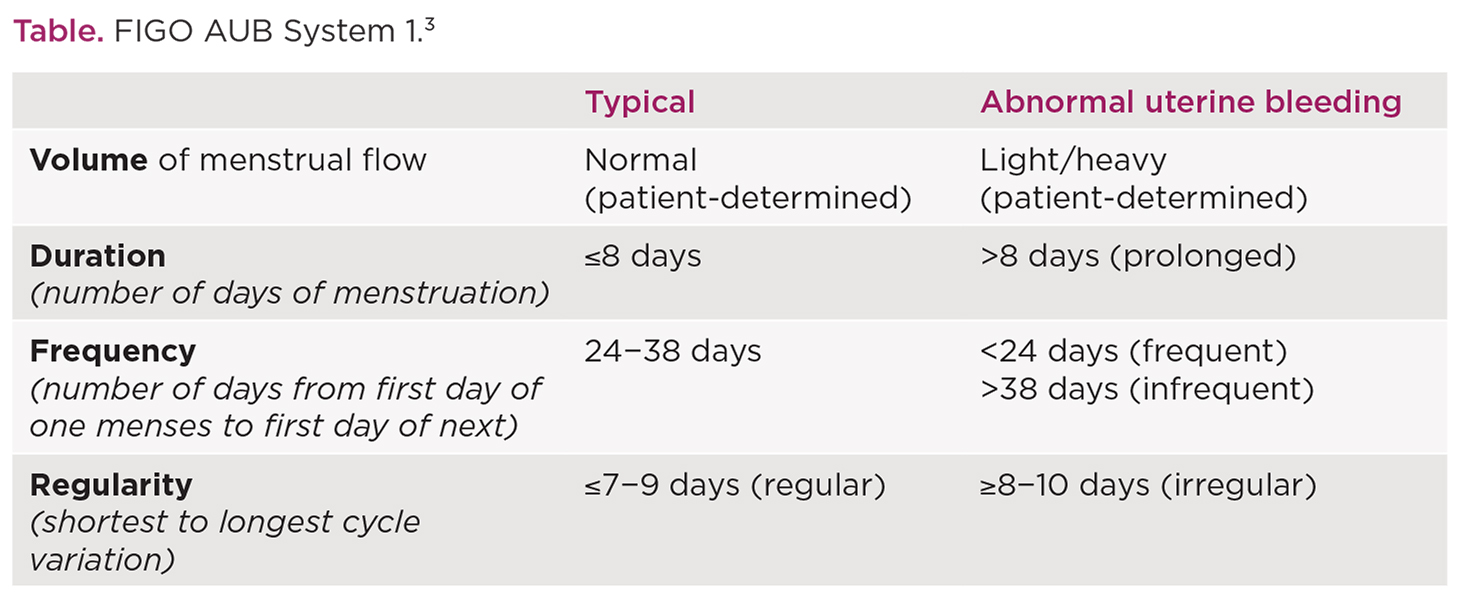
The lack of terminology was addressed by the International Federation of Gynecology and Obstetrics (FIGO) in 2011 (with updates in 2018).3 They recommended assessing menstruation by four main parameters: (i) volume, (ii) duration, (iii) frequency and (iv) regularity, and reviewed the available evidence to define typical and abnormal menstrual bleeding (see Table). The FIGO AUB System 1 provides researchers and clinicians with a set of standardised parameters and simplified terminology (e.g. heavy, prolonged, frequent or irregular menstrual bleeding) to enable global scientific collaboration in menstrual research and to drive clinical excellence.
'Due to the embarrassment and shame that surrounds menstruation, many people do not know what typical menstrual bleeding comprises. This societal problem was previously compounded by a lack of standardised terminology in menstrual research and clinical practice.'
CURRENT TOOLS TO TREAT AUB
There are a range of medical and surgical treatment options available for those experiencing AUB. Selecting appropriate treatments can present challenges for the patient and physician, and requires consideration of the underlying diagnosis, co-morbidities, user preferences and desire for fertility.
The majority of medical treatments are hormonal, acting to override or alter physiological ovarian hormone production. The levonorgestrel-releasing intrauterine system is recommended by NICE for the treatment of heavy menstrual bleeding1 and can be very effective, resulting in amenorrhoea or significant reductions in menstrual blood loss. However, some women will experience intolerable side effects such as irregular, frequent menstrual bleeding or mood changes. Occasionally, the insertion process may be unacceptably painful or can result in uterine perforation, infection or spontaneous expulsion.
Non-hormonal options are limited to non-steroidal anti-inflammatories or the anti-fibrinolytic medication tranexamic acid. These oral medications can be helpful, but are often not effective enough for those with very heavy menstruation.
The most common surgical interventions for abnormal uterine bleeding include endometrial ablation (removal of the womb lining) and hysterectomy (removal of the womb). Hysterectomy can guarantee amenorrhoea but introduces surgical risks of severe blood loss, infection and organ damage.
IDENTIFYING THE CAUSE OF THE PROBLEM
AUB is a symptom and not a diagnosis. Yet, those experiencing menstrual disturbance are often treated without appropriate efforts to identify the underlying cause. The FIGO AUB System 2 provides a practical framework to aid clinicians in establishing a diagnosis.3
The underlying causes of AUB are divided into structural causes (those detectable on examination/imaging) and non-structural causes (normal uterine anatomy).
Structural causes include:
- endometrial Polyps
- Adenomyosis (endometrial-like tissue within the myometrial layer of the uterus)
- Leiomyoma (fibroids) and
- Malignancy (e.g. endometrial).
They are denoted by the acronym PALM.
Non-structural causes (acronym COEIN) include:
- Coagulation disorders
- Ovulatory dysfunction (including perimenopausal bleeding and polycystic ovary syndrome)
- Endometrial causes
- Iatrogenic causes and
- those Not-otherwise classified (e.g. arteriovenous malformations, caesarean scar defects).
APPROPRIATE USE OF CURRENT TOOLS
After detailed history taking and clinical examination, a provisional diagnosis (e.g. AUB-A/E, that is adenomyosis and/or endometrial in origin) should be recorded and further refined by appropriate investigations.
The diagnosis (or diagnoses) should then inform discussions about clinical management. For example, current hormonal treatments are more likely to be effective in those with ovulatory dysfunction than in the patient with a large submucosal leiomyoma (fibroid). Specific, personalised treatments are only possible after accurate diagnosis, e.g. hysteroscopic removal of endometrial polyps (AUB-P) or haematology input and DDAVP treatment (AUB-C).
An accurate diagnosis, good clinical judgement and shared decision making will result in more acceptable, effective treatment of the symptom of AUB.
ADDING TO THE TOOLKIT FOR TREATING AUB
Despite the range of medical and surgical treatment available, many experiencing menstrual disorders are unsatisfied with current options. There is a clear unmet clinical need for better non-hormonal treatments for AUB. The electric lightbulb did not come from the continuous improvement of candles, and AUB presents an opportunity to think outside the box when identifying novel therapeutic targets.
For example, AUB-E is a diagnosis of exclusion, and the exact endometrial aberrations resulting in increased menstrual blood loss remain undefined. Recent research has identified a transient but intense hypoxia in the endometrium during menstruation.4,5 This hypoxia drives repair of the denuded menstrual endometrium to stop menstrual bleeding.4 Those with AUB-E appear to lack this localised tissue hypoxia and have prolonged menstrual bleeding.
Medications are available that mimic the hypoxic response in tissues and these represent an attractive potential therapeutic option to restore endometrial physiology. These treatments would only be required during menstruation and the endometrium is amenable to local delivery methods, creating exciting opportunities for new therapeutic strategies.
ADDRESSING INEQUALITIES BY IMPROVING CLINICAL CARE
AUB can impact education, work, family, finances and mental and physical health. Addressing the problems experienced by those with menstrual disorders will require a truly transdisciplinary approach.6 The role of the specialist menstrual disorders service is to use the currently available tools to their best effect, personalising treatments to restore quality of life. In addition, it is essential to embed menstrual research into clinical practice to develop new and improved options for those facing these debilitating symptoms. Only then can the inequalities experienced by those with AUB begin to be reduced.
Jacqueline A Maybin
Senior Clinical Research Fellow and Honorary Consultant Gynaecologist, MRC Centre for Reproductive Health, University of Edinburgh
REFERENCES
- NICE 2018 Heavy Menstrual Bleeding: Assessment and Management NG88 www.nice.org.uk/guidance/ng88.
- RCOG 2014 National Heavy Menstrual Bleeding Audit Final Report www.rcog.org.uk/globalassets/documents/guidelines/research--audit/national_hmb_audit_final_report_july_2014.pdf.
- Munro MG et al. 2018 International Journal of Gynecology & Obstetrics doi:10.1002/ijgo.12666.
- Maybin JA et al. 2018 Nature Communications 9 295.
- Cousins FL et al. 2016 BMC Research Notes 9 30.
- Critchley HOD et al. 2020 American Journal of Obstetrics & Gynecology 223 624–664.



{kind=link}