Neuroendocrine tumours (NETs) are tumours that occur in cells of the neuroendocrine system, i.e. a network of glands that produce hormones. These can include cells in the pancreas, lung and bowel. NETs are classified as rare. However, their prevalence is increasing, with approximately 4,000 people diagnosed in the UK each year.
NETs are graded based on their severity, from G1 to G3.1 G1 NETs are the lowest grade and have the best prognosis. They are well differentiated and grow slowly. G2 NETs are an intermediate grade, with moderate differentiation and growth. G3 are the highest grade NET with the worst prognosis. They are poorly differentiated, and grow at a high rate. Diagnosis of the correct grade is important to determine the prognosis. Treatments also vary, based on the NET grade. They can include surgery, radiotherapy, chemotherapy or specific targeted treatments such as somatostatin analogues.2
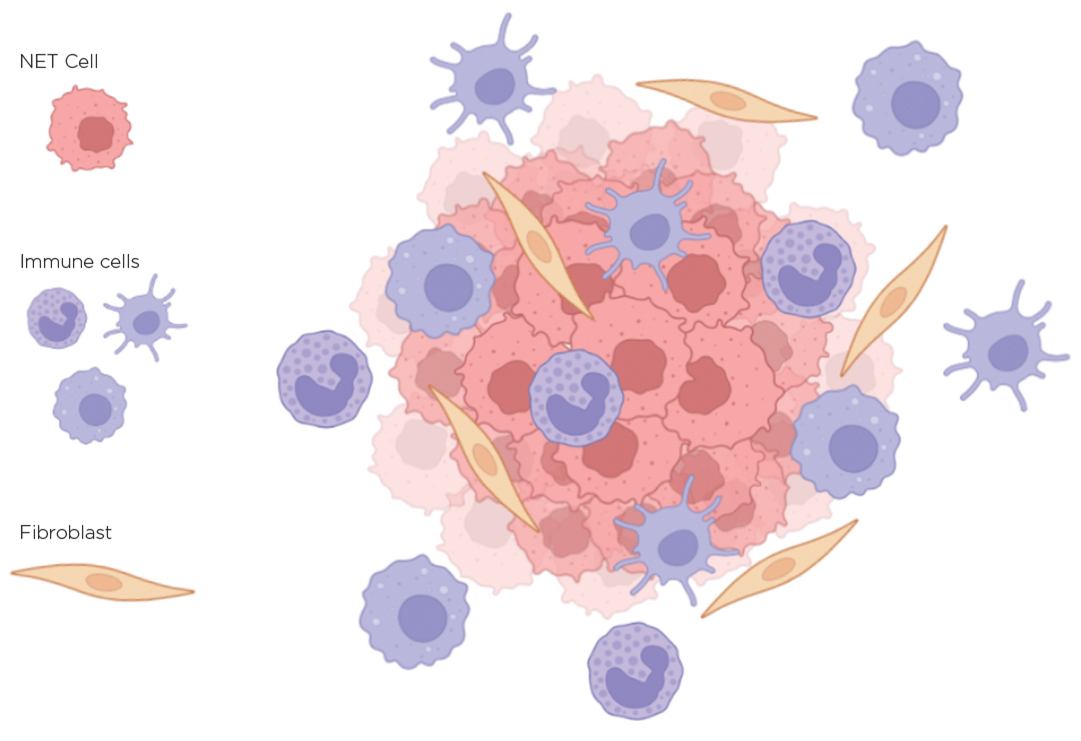
Unsurprisingly, most of the recent research and developments have focused on improving diagnosis and treatment. These include the use of novel technologies to investigate the underlying biology, and the preclinical development of new therapies, as well as the evaluation of novel agents in clinical trials. In particular, studies have included identification of changes in the cellular environment (known as the microenvironment) of the NETs (see Figure),3,4 not just the tumour cells themselves.

The NET microenvironment. Created by the author using BioRender
TECHNOLOGICAL PROGRESS
One of the most recent technological advances is the ability to assess gene expression changes at the single cell level, using single cell RNA sequencing (scRNA-Seq). This means that specific expression patterns can be observed in individual cells within a tumour, which can also be used to determine the different cell types present. This technology has already been used for multiple cancers but, more recently, it has been used to assess NETs, including those from the pancreas, lung and pituitary.
For example, a study in pancreatic NETs revealed the presence of immune cells and fibroblasts, as well as the NET cells, and identified a gene signature that could predict the malignant potential of the NET cells.5 This study also showed that the microenvironment of the NET is very different to that surrounding metastatic tumour sites. This increased biological understanding can help in making treatment decisions, especially if you know that the NET and the metastatic tumour may respond differently to the treatments given.
The gene signature can also be used to aid diagnosis or as a biomarker. It was recently reported that the presence of circulating tumour cells in the blood of patients with a pancreatic NET could be used as biomarkers to categorise patients in clinical practice and trials.6 This involves taking blood samples and isolating the tumour cells that are present within them.
Combining the single cell sequencing technology with the technology to isolate circulating tumour cells to look for malignant expression patterns could provide a particularly powerful diagnostic or prognostic tool.
LABORATORY MODELS
'Using technologies and models to investigate the whole tumour environment, rather than just the tumour cells themselves, has highlighted a number of other possible therapeutic targets.'
One of the biggest disadvantages of technologies like scRNA-Seq is the requirement for substantial amounts of patient material. Therefore, a challenge in NET research has always been to develop good laboratory models that accurately represent the tumours seen in patients. Cell lines are often used; however, they grow on 2D surfaces and exist as single cells, rather than as clusters of cells like the tumours in patients.
To overcome this, organoid models have been developed. These are 3D cell culture models that are established from patient tissues, and represent the tumours more closely than traditional cell lines, as they include many cell types that are present (including immune cells). A collection of NET organoid models was recently established.7 This consists of lung, oesophagus, stomach, liver, biliary tract, pancreas, duodenum and colon organoids. All of these were comprehensively examined for genetic mutations, and gene expression changes. These have therefore provided a model to further examine the biology of NETs, and also have the potential to be used for the assessment of novel drugs.
THERAPEUTIC TARGETS
Using technologies and models like those mentioned above to investigate the whole tumour environment, rather than just the tumour cells themselves, has highlighted a number of other possible therapeutic targets.
One of particular interest recently is the immune system. Immunotherapy has shown great results in many cancer types, and has revolutionised cancer treatment. Clinical trials evaluating immunotherapy (consisting of antibodies targeting different immune-associated elements) have been undertaken in in NETS, but have had mixed results.8
Using immunotherapy alone appears to have a very limited effect, except in lung NETs where modest response rates have been reported with immune checkpoint inhibitors.9 The use of two immunotherapy drugs in combination has, however, shown more promising results. For example, the combination of anti-CTLA-4 and anti-PD1 antibodies showed a response to the treatment in up to 44% of patients with high grade NETs.10
There is still a long way to go to determine if these drugs will have a use in patients with a NET, but the continuing research into the NET immune environment, as well as the development of better biomarkers to determine response rates, will help determine which patients should receive these drugs, and provide better methods to monitor their progress.
Overall, these are exciting times for NET research, and hopefully these scientific and medical advances will come together to improve patient care in the near future.
Kate Lines
Oxford-BMS Research Fellow, OCDEM, University of Oxford
REFERENCES
1. Rindi G et al. 2018 Modern Pathology 31 1770–1786.
2. Zandee WT & de Herder WW 2018 Neuroendocrinology 106 357–365.
3. Marques P et al. 2020 Frontiers in Neuroendocrinology 58 100852.
4. Takkenkamp TJ et al. 2020 Endocrine-Related Cancer 27 R329–R343.
5. Zhou Y et al. 2021 International Journal of Biological Science 17 3760–3775.
6. Mandair D et al. 2021 Journal of Clinical Endocrinology & Metabolism 106 872–882.
7. Kawasaki K. et al. 2020 Cell 183 1420–1435.
8. Garcia-Alvarez A et al. 2022 Current Oncology Reports 24 451–461.
9. Sherman S et al. 2020 Lung Cancer 143 40–46.
10. Patel SP et al. 2020 Clinical Cancer Research 26 2290–2296.



{kind=link}