It was just after 6.30 p.m. when John Pickard (now Emeritus Professor of Neurosurgery at the University of Cambridge) leaned over and asked, “Surely there must be another way to locate these?”
We were sitting in the pituitary multidisciplinary team meeting, discussing the final case and peering hard at the screen, in the hope of discerning where the corticotroph adenoma was hiding. At the time, John was the lead pituitary surgeon in Cambridge, with extensive experience of transsphenoidal surgery. Perhaps just as importantly, he was Academic Head of Department and Director of the Wolfson Brain Imaging Centre, recognised for its pioneering work in traumatic brain injury and the use of positron emission tomography (PET) imaging.
And so began the journey to establish a molecular (functional) pituitary imaging service for UK patients, with two primary aims: (i) to improve the localisation of small microadenomas (‘picoadenomas’, to quote the distinguished pituitary neuroradiologist Jean-François Bonneville) and (ii) to more reliably discriminate residual or recurrent tumour from post-treatment remodelling after primary therapy.
WHY WAS NO ONE USING PET?
In the initial phase of the project, the obvious question to ask was why nobody was using PET to localise pituitary adenomas. After all, endocrinologists are very comfortable with functional imaging in other disease areas, e.g. thyroid scintigraphy, parathyroid single photon emission computed tomography/computed tomography (SPECT/CT), 68Ga-dotatate PET/CT.
On reviewing the literature, it became clear that several attempts had been made to find a suitable functional imaging strategy, but that each had encountered challenges.
First, which ligand should be preferred? 18F-fluorodeoxyglucose (18F-FDG), with its central role in clinical oncology, is readily available, but pituitary adenomas show very variable (even absent) tracer uptake. At the same time, avid 18F-FDG uptake in adjacent brain tissue can confound scan interpretation. Other more selective ligands (e.g. those targeting somatostatin or dopamine receptor expression) inevitably have more restricted usage, meaning that a panel of ligands would be required to image different pituitary adenoma subtypes.
Secondly, attempts to precisely localise sites of tracer uptake were hampered by the lack of spatial resolution of scintigraphy and SPECT/CT, and even PET/CT has limitations, given the modest structural information provided by CT when compared with magnetic resonance imaging (MRI) of the sella and parasellar regions.
IDENTIFYING ANOTHER METHOD
'In the initial phase of the project, the obvious question to ask was why nobody was using PET to localise pituitary adenomas.'
This prompted us to consider an alternative approach. A common property of most pituitary adenomas is peptide synthesis, even in clinically non-secretory tumours (as evidenced by immunohistochemical staining and in vitro cultures of resected tumours).1 We therefore selected 11C-methionine, which is taken up via the L-type amino acid transporter 1 (LAT1), as a ‘universal’ PET tracer (Met-PET). This was based on previous pilot studies that had confirmed uptake in different pituitary adenoma subtypes.
In parallel, colleagues in nuclear medicine, radiology and medical physics optimised algorithms to enable Met-PET/CT to be coregistered with volumetric (1-mm slice thickness) MRI to create hybrid images (Met-PET/MRCR), that allow more accurate localisation of sites of tracer uptake through precise correlation with anatomical findings.
METHODOLOGY IN PRACTICE
So what is the experience to date with >700 scans performed in studies and clinical practice?
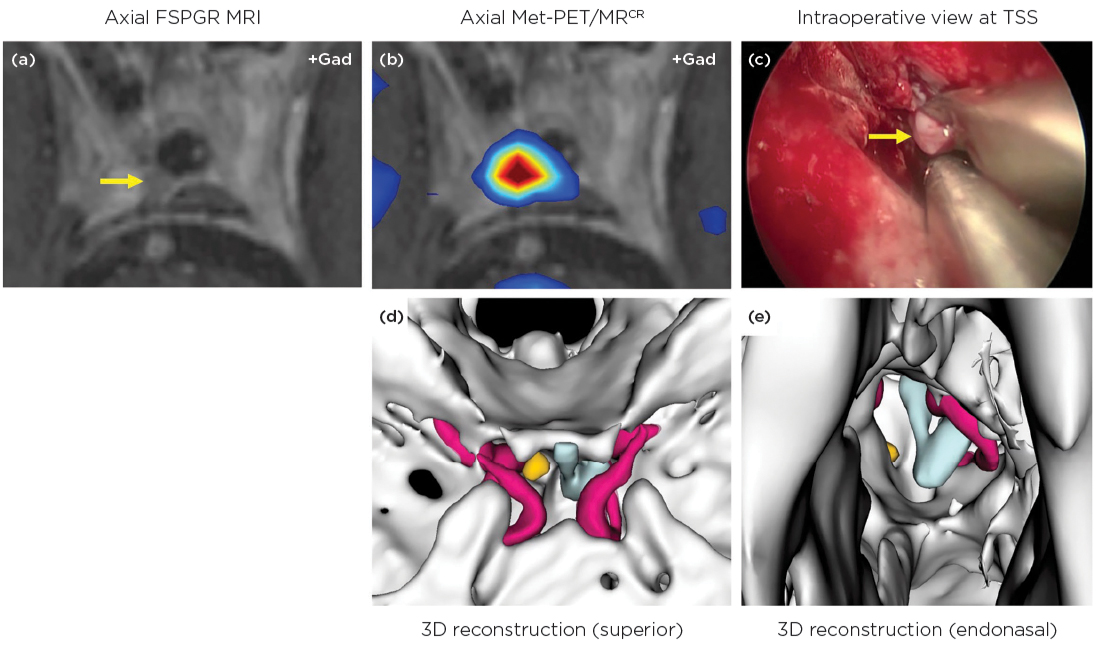
In acromegaly, Met-PET/MRCR can help confirm suspected, or reveal unexpected, sites of residual disease following primary treatment (see Figure).2 It can also provide key information about the degree of parasellar involvement, to permit repeat transsphenoidal surgery in patients previously considered to have unresectable lateral tumour extension.3 In Cushing’s disease, both de novo and recurrent corticotroph adenomas may be more readily visualised with Met-PET/MRCR when MRI is indeterminate or negative.4
'while MRI will remain the cornerstone of pituitary imaging in most patients, the advent of molecular imaging means that more patients can now be considered for definitive treatment (surgery or radiosurgery).'
Although microprolactinomas are traditionally managed with medical therapy, several groups have recently demonstrated comparable or superior outcomes following transsphenoidal surgery.5 With increasing awareness that a significant proportion of patients experience intolerable side effects when treated with dopamine agonists (including impulse control disorder), the role of surgery is being re-evaluated.6 In this setting, Met-PET/MRCR has a potentially important role to play in patients with inconclusive MRI, because prolactinomas are 11C-methionine-avid and therefore readily visualised. This can permit targeted selective adenomectomy without the need for more extensive exploration of the gland (Bashari et al. unpublished observations).
Studies in the rarest pituitary adenoma subtype, thyrotroph adenomas, have also allowed development of novel approaches. These include subtraction imaging, in which PET is performed before and after endocrine treatment to suppress tumour activity. This has particular value in microadenomas which are not clearly seen on MRI. Here, normalisation of thyroid function tests following somatostatin receptor ligand therapy correlates with extinction of the focus of 11C-methionine uptake at the site of the tumour.7
[Figure shows: Met-PET/MRCR in a patient with persistent acromegaly despite previous transsphenoidal surgery (TSS) on two occasions, radiotherapy (10 years
earlier) and maximal somatostatin receptor ligand therapy. (a, b) Although no residual tumour could be visualised on standard coronal and sagittal
images, Met-PET/MRCR revealed an area of focal tracer uptake that could be appreciated on axial volumetric MRI (arrow). (c) At surgery, a small
focus of residual tumour was resected (arrow) from the site identified on Met-PET/MRCR. (d, e) 3D reconstructed images using PET, CT and MRI
datasets, showing the position of the remnant adenoma (yellow) relative to the residual normal gland (turquoise) and intracavernous carotid
artery (red). FSPGR, fast spoiled gradient recalled echo; Met-PET/MRCR, 11C-methionine PET co-registered with volumetric (FSPGR) MRI.]
OTHER IMPLICATIONS
Finally, combining data from multiple imaging modalities enables detailed 3D reconstructions of the sella and parasellar regions (Figure). This has the potential for incorporation into surgical planning and training and, at the same time, may facilitate patient understanding of a planned procedure, for example through 3D printing of individual patient models.8 So, while MRI will remain the cornerstone of pituitary imaging in most patients, the advent of molecular imaging means that more patients can now be considered for definitive treatment (surgery or radiosurgery).9
Olympia Koulouri
Clinical Lecturer in Endocrinology, Institute of Metabolic Science, University of Cambridge & Addenbrooke’s Hospital, Cambridge
Waiel Bashari
Consultant Endocrinologist, Institute of Metabolic Science, Addenbrooke’s Hospital, Cambridge
Mark Gurnell
Professor of Endocrinology, Institute of Metabolic Science, University of Cambridge & Addenbrooke’s Hospital, Cambridge
REFERENCES
1. Hanson PL et al. 2005 European Journal of Endocrinology 152 363–370.
2. Koulouri O et al. 2016 European Journal of Endocrinology 175 485–498.
3. Bashari WA et al. 2020 Neurosurgical Focus 48 E8.
4. Koulouri O et al. 2015 European Journal of Endocrinology 173 M107–M120.
5. Zamanipoor Najafabadi AH et al. 2020 Journal of Clinical Endocrinology & Metabolism 105 e32–e41.
6. Honegger J et al. 2020 Pituitary 23 45–51.
7. Koulouri O et al. 2016 Lancet Diabetes & Endocrinology 4 1050.
8. Gillett D et al. 2021 3D Printing in Medicine 7 24.
9. Bashari WA et al. 2021 Journal of Nuclear Medicine 62 57S–62S.


{kind=link}