Thyroid disorders are one of the most common causes for referral to the endocrinology outpatient clinic. This process has been managed using guidelines which are regularly updated. The main points of reference for decisions regarding the management of thyroid disease are NICE Clinical Knowledge Summaries and resources provided by the British Thyroid Association, the European Thyroid Association and the American Thyroid Association. These usefully guide the clinician in decisions regarding treatment, which can then be further tailored to a patient’s clinical presentation.
NICE Guideline 145 is the UK’s most recently updated compendium, including treatment for patients with either hyperthyroidism or hypothyroidism, using evidence from most recent research studies and clinical trials.
Management can vary depending on the age of the individual affected. There are variations for pregnancy and childhood, as well as acceptance of conservative approaches in situations where more radical therapy may prove counter-productive or potentially adversely affect the quality of life of the individual concerned.
'Thyroid disorders are one of the most common causes for referral to the endocrinology outpatient clinic.'
Rather than going through each individual guideline, the focus here will be to try and provide a concise summary of the various guidelines in their latest iterations. There were some disruptions to normal service due to COVID, but these have now started to normalise.
HYPERTHYROIDISM
Hyperthyroidism is mostly managed in secondary care by endocrinologists and endocrine specialist nurses with an interest in thyroid disease.
Initial investigations and management should involve taking a good history and identification or ruling out of the presence of thyroid eye disease and any other systemic effects of thyroid hormone excess.
Antithyroid hormone medications, such as propylthiouracil and methimazole/carbimazole, can be commenced in the first instance. Thyrotrophin receptor antibodies are an important diagnostic tool in differentiating between autoimmune thyrotoxicosis and transient hyperthyroidism, which can occur in post-viral situations or in the early inflammatory stages of autoimmune hypothyroidism.1
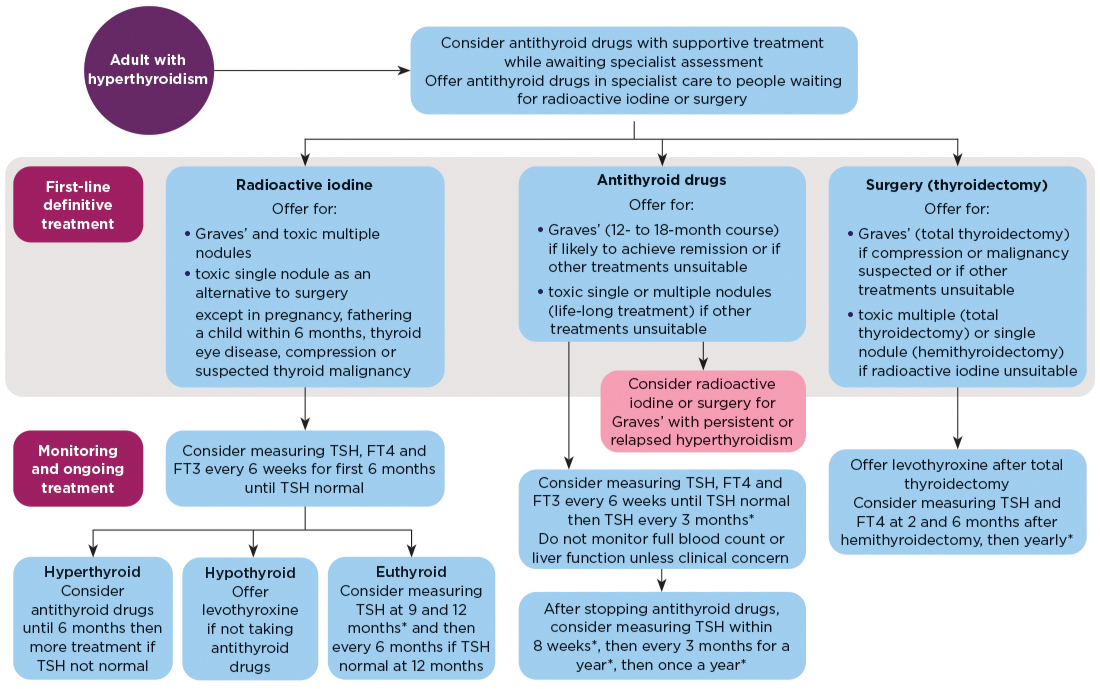
In a departure from the previous approach, NICE recommends discussing the use of radioactive iodine (RAI) with patients during the first consultation. The indications for RAI are Graves’ disease and toxic multiple nodules or toxic single nodule, as an alternative to surgery; the exceptions are cases of pregnancy, fathering a child within 6 months, thyroid eye disease, compression or suspected thyroid malignancy. Otherwise, the recommendation remains for 12–18 months of antithyroid drugs, but leaving the door open for RAI or surgery in the event of hyperthyroidism which is difficult to control.2
Surgery should also be discussed in the event of any evidence of compression on local structures or suspected/confirmed malignancy.
NICE has provided a summary sheet for quick guidance on management. This includes monitoring post-RAI or surgical definitive treatment (see Figure).

Hyperthyroidism in adults: management and monitoring. FT3, free tri-iodothyronine; FT4, free thyroxine; TSH, thyrotrophin. *With cascading – measuring FT4 in the same sample if TSH is above the reference range, and FT4 and FT3 in the same sample if TSH is below the reference range. ©NICE 2019
There have also been updates to the recommended periods of observation for monitoring and treatment of subclinical hyperthyroidism. Such patients may be discharged if their levels remain stable, with no evidence of cardiovascular/metabolic pathologies after six months or two subsequent stable levels. When in doubt, it is advised to recheck the levels using a different laboratory, to ensure standardisation of reporting and rule out assay interference.
The European Group on Graves’ Orbitopathy has recently published updated guidelines for the management of thyroid orbitopathy. The focus is on ensuring a multidisciplinary team approach and use of pulse intravenous methylprednisolone. Other second-line treatments that are advised include a combination of oral steroids with azathioprine or cyclosporine, teprotumumab, tocilizumab or rituximab. These will all need a specialised approach. In mild cases, the use of selenium is recommended for patients in selenium-deficient regions. These treatments may need to be combined with local steroid injections and/or orbital radiotherapy. RAI is to be used in caution in Graves’ orbitopathy.3
HYPOTHYROIDISM
Treatment and management of hypothyroidism have predominantly migrated to the remit of primary care, with secondary care involvement only in certain scenarios.
The cut-off for a raised thyrotrophin at which treatment is recommended has been established at ≥10mIU/l on two separate occasions three months apart.
The recommended starting dose for levothyroxine, as per NICE, is 1.6µg/kg in the absence of cardiovascular disorders, and needs to be adjusted to the nearest 25µg dose for dispensing purposes.
NICE does not recommend routinely offering liothyronine or offering natural thyroid hormone extracts in the treatment of hypothyroidism. This statement has naturally sparked debate, but the recommendation is based on current available clinical research, which does not support the use of these medications.
However, as per the European Thyroid Association guidelines, a supervised trial may be considered after careful discussions with patients about expectations, with a clearly defined time frame to monitor for any response. The recommendation also states that this could be considered in patients who have hypothyroidism and have not had symptomatic relief, despite optimal attempts with standard levothyroxine therapy. However, it should not be offered if the patient is pregnant, and must be done with caution in the elderly.4
None of the major thyroid associations routinely recommend liothyronine.
Monitoring thyroid hormone replacement can be done using thyrotrophin as a tool for guidance, and titrating the dose based on this.
'Management can vary depending on the age of the individual affected. There are variations for pregnancy and childhood, as well as acceptance of conservative approaches in situations where more radical therapy may prove counter-productive.'
THYROID DISEASE IN OTHER SCENARIOS
Contrast media
The European Thyroid Association has issued new guidance on thyroid function abnormalities induced by iodine-based contrast media. Essentially, the recommendations provide advice on treatment and follow up, but dissuade from screening pre-scan, as it has no benefit. Treatment is only indicated when the thyroid dysfunction persists for a prolonged period, or in elderly patients with heart disease. There are no absolute monitoring recommendations, but thyroid dysfunction lasting for longer than two or three months after contrast administration will probably need treatment.5
Fertility
The latest European Thyroid Association guidelines suggest routine testing for mothers with reduced fertility, and aiming for an optimum level of thyrotrophin <2.5mIU/l. Information regarding the use of levothyroxine in patients undergoing artificial reproductive methods mainly focuses on aiming to improve success rates if patients have thyrotrophin >4.0mIU/l.6
Venkatram Subramanian
ST6 Diabetes and Endocrinology, North West England, East Lancashire NHS Foundation Trust
Society Endocrine Ambassador
Article amended on 23 June 2022 to clarify reference to the NICE guidelines on prescribing liothyronine for primary hypothyroidism.
REFERENCES
1. Kahaly GJ et al. 2018 European Thyroid Journal 7 167–186.
2. NICE 2019 Thyroid Disease: Assessment and Management NG145.
3. Bartalena L et al. 2021 European Journal of Endocrinology 185 G43–G67.
4. Jonklaas J et al. 2021 European Thyroid Journal 10 10–38.
5. Bednarczuk T et al. 2021 European Thyroid Journal 10 269–284.
6. Poppe K et al. 2021 European Thyroid Journal 9 281–295.


{kind=link}