The role of the pharmacist has developed considerably over the past 20 years, with an increase in opportunities to work directly at the clinical ‘coalface’, as well as maintaining the backbone of medication procurement and dispensing in the NHS.
There are a considerable number of differing roles that pharmacists can undertake post-qualification, but the general direction is towards greater autonomous clinical practice. New regulations came into place in 2021 that stipulate that, from 2026, all pharmacists will be independent prescribers at qualification. Over the past 10 years, the development of pharmacists working clinically in secondary care and general practice settings has become far more structured and is now closely aligned to the physician model.
'The first consultant pharmacist nationally in endocrinology and diabetes was approved and appointed in 2017, with two further consultant pharmacist posts specifically in diabetes following in 2019 and 2021.'
CAREER STRUCTURE
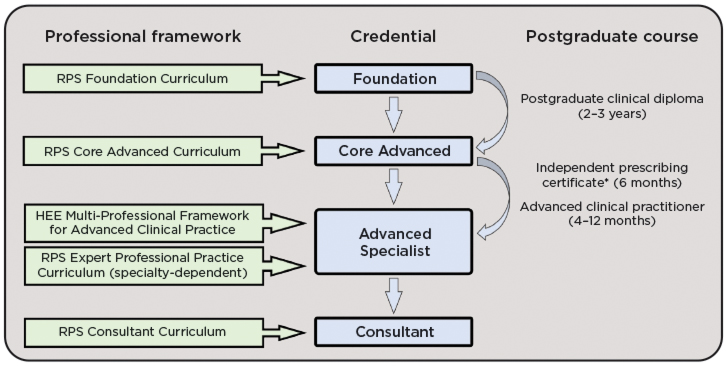
Pharmacists working in hospitals will spend two to three years post-qualification undertaking a postgraduate clinical diploma, with the development of a portfolio of evidence towards core advanced (generalist) competencies. If choosing a clinical specialist career path, such as endocrinology, they will then embark upon developing advanced competencies and have assessment against the advanced specialist framework, with the possibility of developing and mapping competencies against a consultant level framework (see Figure).
The title of ‘Consultant Pharmacist’ has far greater restriction than many other professions, with both the consultant pharmacist post itself having to be assessed and approved by the Royal Pharmaceutical Society, and a personal development portfolio being submitted for national assessment across four pillars of consultant practice: clinical practice, leadership, education and research.1

Clinical pharmacist credentialing and professional progression pathway.7 HEE, Health Education England; RPS, Royal Pharmaceutical Society. *New regulations came into place in 2021 stating that all pharmacists qualifying by 2026 will be independent prescribers on qualification.
THE CASE FOR CHANGE
There has been a gradual increase in the number of pharmacists working nationally in endocrine services, which is expected to follow the same trajectory as secondary care diabetes services, with many more now employing a specialist pharmacist. The first consultant pharmacist nationally in endocrinology and diabetes was approved and appointed in 2017, with two further consultant pharmacist posts specifically in diabetes following in 2019 and 2021.
Endocrine services, now more than ever, need to increase service capacity and utilise the full multidisciplinary team (MDT) that is available. The mind initially drifts towards the obvious support a pharmacist could give to a service with frequent medication shortages, rare and high-cost medications, home care solutions and inpatient medication safety, but they can also be supported to develop as an autonomous clinical practitioner, as a permanent member of the clinical team.
CASE STUDY 1: CONSULTANT PHARMACIST
The consultant post was developed at University Hospital Southampton NHS Foundation Trust, a large tertiary endocrine centre. The post had a similar job plan to a medical consultant, with seven programmed activities (PAs) in direct clinical care and three PAs of supporting professional activities, which include regional and national diabetes and endocrine work. The post was created as 50:50 diabetes and endocrinology, with a mixture of inpatient and outpatient activity.
Regarding endocrinology, the consultant pharmacist works as an autonomous clinical consultant with their own consultant clinic codes, responsible for organising, interpreting, prescribing and following up on endocrine investigations. All referrals are triaged by a medical consultant within the service, and cases listed for the consultant pharmacist are a good mixture of general endocrinology. This releases consultant physician time to focus on more tertiary centre specialist activity, so increasing service capacity on a number of fronts. In addition, the consultant pharmacist assists specialist registrars with inpatient endocrine queries and oversight of outpatient clinics alongside consultant medical colleagues.
Working in a tertiary centre, the consultant pharmacist also supports the pituitary, adrenal, neuroendocrine and joint biochemistry MDTs, with a particular focus on complex case management. They have supported the development of joint working initiatives with oncology and neurology around the increase in monoclonal antibody-related endocrinopathies. Since January 2020, the consultant pharmacist has taken on the clinical director role within the diabetes and endocrine service, and undertakes all activities associated with this role, including consultant job planning. They have driven service development in areas such as andrology and male infertility, adrenal MDT pathways and non-diabetic hypoglycaemia.
CASE STUDY 2: SPECIALIST ENDOCRINE PHARMACIST
A specialist pharmacist for endocrinology can be trained to effectively self-manage significant cohorts of patients within specialist endocrine services. Case 2 describes a pharmacist appointed and embedded within a district general hospital where they now manage 25–30% of all endocrine outpatients within the service, focusing mainly on hyperthyroidism and adrenal incidentalomas.
Approximately 10% of patients are referred with adrenal incidentalomas, which are investigated using a standard protocol. However, multiple medications interfere with these investigations, particularly an aldosterone:renin ratio.2 Switching to non-interfering medications whilst managing blood pressure can be difficult, but is routinely and confidently undertaken by experienced endocrine pharmacists. The pharmacist also manages this section of the adrenal MDT, deciding which patients should be discussed on each occasion, so that they are safely managed and have input from all the necessary specialists, including endocrinologists, radiologists and biochemists. Patients who are diagnosed with an active nodule can be transferred to consultant care as needed. and referred back to the pharmacist for ongoing monitoring, once a treatment plan is in place.
The endocrine pharmacist also supports the department through arranging the supply of hydrocortisone emergency kits for patients who have adrenal insufficiency, as well as education and training on sick day rules and when to use the kit.
From an inpatient perspective, admissions to hospital frequently result in missing or altered regular medications, such as long term steroids, and simple nasal sprays like desmopressin can be overlooked. Endocrine pharmacists support the development of the whole pharmacy workforce to create a staff group that is refocused on medications safety within the area of endocrinology. They are also able to provide education to different staff groups across the Trust, to identify high risk and vital medications, and empower staff to detect and resolve any issues quickly, for the safety of patients.
CASE STUDY 3: PAEDIATRIC ENDOCRINE SPECIALIST PHARMACIST
The national clinical standards for paediatric endocrinology require a nominated paediatric pharmacist for lead specialist centres.3 Despite this, the role of the paediatric endocrine pharmacist remains under-utilised nationally.
Children have unique pharmaceutical needs that pose two challenges to the clinician. First, there is genuine scarcity of an evidence base behind pharmacological management in children: hydrocortisone dosing in paediatric adrenal insufficiency and drugs for paediatric obesity are current hot topics and case examples. Secondly, children are a heterogenous group, with individual needs that often necessitate critical examination of the drug formulation being offered, its clinical appropriateness, practicality and cost-effectiveness.
In 2021, the pharmacist revived steroid medication review clinics, discussing medicine adherence, educating families on sick day rules, and training parents on emergency hydrocortisone injections. The aspect uniquely provided by the pharmacist was a review of hydrocortisone formulations: assessing the children’s individual abilities and level of independence, discussing the available options with parents, and prescribing a different formulation as each child ‘outgrows’ their current one. With two recent national alerts on use of hydrocortisone formulations in children,4,5 this task requires a practitioner experienced in both paediatrics and pharmaceutical care.
'Considering the future needs of the endocrine workforce, we must consider utilising the full MDT, where pharmacists also evolve into being a core member of every endocrine team.'
An example within a different setting is a pharmacist-led review of zoledronate day cases. The pharmacist is trained to assess the patient’s history of fractures before each infusion, to prescribe zoledronic acid, pre-medication and discharge medicines, and then to carry out a bedside consultation to review the patient’s management of bone disease through medication and diet. The new model allowed identification of patients on suboptimal vitamin D therapy, switching to more suitable calcium formulations to match the individual children’s needs, and counselling on management of acute phase reaction post-infusion.
Another opportunity for pharmacists to provide support is in childhood obesity. In the UK, this has risen at an alarming rate, with one in four children now being obese at the time they leave primary school.6 Given the early emergence of co-morbidities in this population, there is an urgent need for specialist practitioners in this field. In Southampton, the pharmacist works within the tier 3 service to use glucagon-like peptide-1 (GLP1) agonists for paediatric obesity. The role involves patient education on subcutaneous injection administration, pharmacist-led GLP1 review clinics, and independent prescribing for the service.
IN CONCLUSION
With the increase in ‘advice and guidance’ requests for endocrinology that has been seen over the past three years, service backlogs due to COVID-19, and a general increase in referrals into the specialty, greater senior clinician activity is needed in endocrine services. Nowadays, most endocrine services could not function without their specialist nursing team. However, considering the future needs of the endocrine workforce, we must consider utilising the full MDT, where pharmacists also evolve into being a core member of every endocrine team.
Philip Newland-Jones
Consultant Pharmacist Diabetes & Endocrinology and Clinical Director Diabetes & Endocrinology, Honorary Senior Clinical Lecturer, University Hospital Southampton NHS Foundation Trust
Hannah Smurthwaite
Specialist Endocrinology Pharmacist, Kettering General Hospital
Nabil Boulos
Specialist Pharmacist Paediatric Endocrinology and Diabetes, Southampton Children’s Hospital
REFERENCES
1. Department of Health 2020 Consultant Pharmacist Guidance www.hee.nhs.uk/sites/default/files/documents/Consultant%20Pharmacist%20Guidance%20Final%20Jan2020.pdf.
2. Funder et al. 2016 Journal of Clinical Endocrinology & Metabolism 101 1889–1916.
3. British Society for Paediatric Endocrinology and Diabetes 2019 UK Standards for Paediatric Endocrinology www.bsped.org.uk/media/1580/uk-standards-for-paediatric-endocrinology-2019.pdf.
4. MHRA 2018 Drug Safety Update www.gov.uk/drug-safety-update/hydrocortisone-muco-adhesive-buccal-tablets-should-not-be-used-off-label-for-adrenal-insufficiency-in-children-due-to-serious-risks.
5. MHRA 2021 Drug Safety Update www.gov.uk/drug-safety-update/alkindi-hydrocortisone-granules-risk-of-acute-adrenal-insufficiency-in-children-when-switching-from-hydrocortisone-tablet-formulations-to-granules.
6. NHS Digital 2021 National Child Measurement Programme, England 2020/21 School Year https://digital.nhs.uk/data-and-information/publications/statistical/national-child-measurement-programme/2020-21-school-year.
7. Royal Pharmaceutical Society 2022 Credentialing: Setting the Standards for Pharmacy www.rpharms.com/development/credentialing.



{kind=link}