Jackie Maybin provides a synopsis of her
Early Career Prize Lecture on hypoxia in menstrual physiology and pathology.
1
The presence of endometrial hypoxia at the time of menstruation was suggested over 70 years ago, but has remained a topic of intense debate ever since. Determining the presence and role of hypoxia in menstrual physiology will increase our understanding of the mechanisms of repeated, scar-free, endometrial injury and repair which occur monthly during a woman’s reproductive lifetime. In addition, it may identify new therapeutic strategies for women suffering from common and debilitating menstrual disorders.
A CLINICAL PROBLEM
One in three women will experience heavy menstrual bleeding (HMB) during their lifetime. HMB can result in severe anaemia and has a significant negative impact on quality of life. It is estimated that 5 million work days are lost each year in the UK due to menstrual problems, resulting in a huge socio-economic cost.
Current medical therapies have many hormonal side effects, meaning otherwise healthy women are proceeding to risky, fertility-removing surgery. There is a clear unmet need for new medical treatments. These can only be developed by delineating endometrial physiology and identifying the aberrations that occur in women with HMB.
THE PHYSIOLOGY OF MENSTRUATION
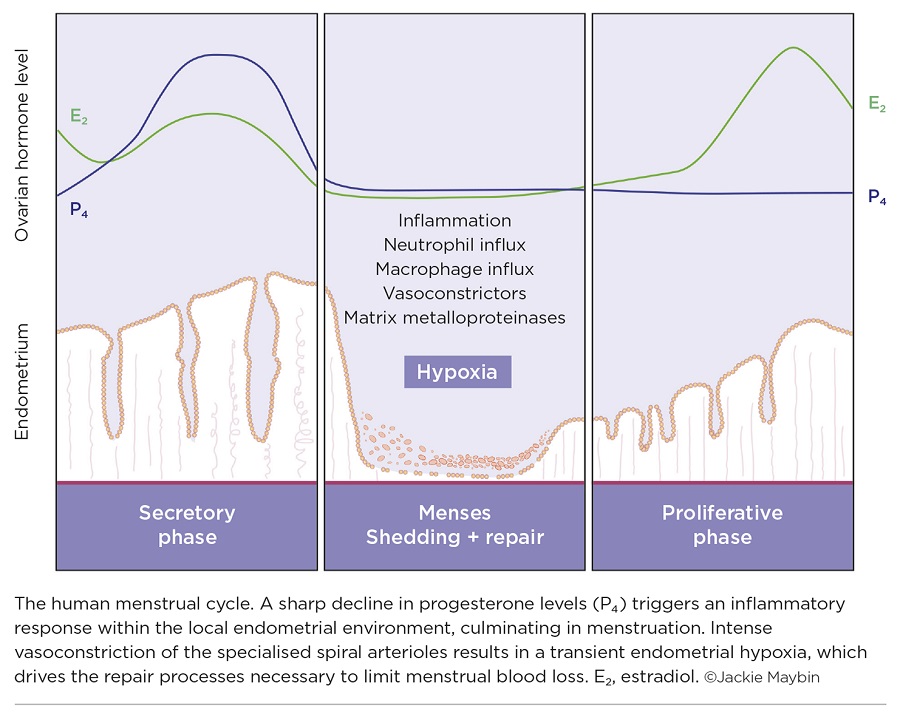
In the absence of pregnancy, the corpus luteum regresses and there is a dramatic decline in progesterone levels. This progesterone withdrawal is the trigger for menstruation (Figure). There is an increase in endometrial inflammatory mediators and an influx of innate immune cells to the local environment. Vasoconstrictors are also increased at this time, including prostaglandin F2α and endothelin-1, to reduce endometrial arteriole diameter and limit menstrual blood loss.
This endometrial inflammatory cascade culminates in activation of matrix metalloproteinases. These enzymes degrade the extracellular matrix, initiating shedding of the upper two-thirds of the endometrium during menstruation. The resulting denuded endometrial surface must repair efficiently to limit menstrual blood loss and to regain endometrial function, i.e. facilitate implantation if fertilisation occurs. The regulation and mechanisms of this repeated, scar-free, endometrial repair are not well understood.
THE PRESENCE OF HYPOXIA IN THE ENDOMETRIUM
In the 1940s, Markee transplanted human endometrial tissue into the anterior chamber of the rhesus monkey eye. This allowed direct visualisation of endometrial changes after administration of progesterone and subsequent withdrawal. Intense vasoconstriction of endometrial spiral arterioles was visualised, compatible with tissue hypoxia following progesterone withdrawal.2
However, since this observation, the presence and role of hypoxia in the endometrium have remained the subject of debate in the reproductive literature. In vitro culture of primary stromal cells and ex vivo culture of endometrial explants revealed that hypoxia did not increase levels of matrix metalloproteinases, suggesting that hypoxia is not involved in endometrial breakdown.3,4
A mouse xenograft model also failed to detect hypoxia during endometrial breakdown or repair. In this model, fragments of functional endometrium were xenografted to ovariectomised, immunodeficient mice, which were then exposed to sequential oestradiol and progesterone prior to withdrawal of ovarian hormones.5 However, disturbance of endometrial vascular architecture and the immunodeficiency necessary for maintenance of this model will have had a considerable impact on menstrual physiology.
We hypothesised that hypoxia was present in the menstrual endometrium and that it is necessary for normal endometrial repair of the denuded endometrial surface following shedding.
We examined well-categorised human endometrial tissue collected from women at different stages across the menstrual cycle. Hypoxia inducible factor (HIF) is the master regulator of the cellular response to hypoxia. It is composed of two subunits: alpha (HIF-1α) and beta (HIF-1β). HIF-1α is regulated by oxygen and is rapidly degraded by the proteasome in normoxic conditions. Therefore, its presence is a marker of hypoxia. We revealed that HIF-1α is present in the human endometrium exclusively following progesterone withdrawal, with maximal levels during menstruation. Downstream targets of HIF-1α were also increased in the endometrium during menstruation.
To confirm the presence of hypoxia at menstruation, we artificially induced mice to have periods by giving them injections of oestrogen and progesterone to mimic the hormone fluctuations experienced by women. Pimonidazole (HydroxyprobeTM) is a marker that detects tissue oxygen levels below 10mmHg. Pimonidazole staining was present in the endometrium of mice during active menstrual bleeding, but had completely resolved when endometrial repair was complete.
HYPOXIA’S ROLE
Our human and mouse studies detected hypoxia in the menstrual endometrium; but what role does it play in endometrial function? Women with HMB had significantly less endometrial HIF-1α protein during menstruation than women with normal blood loss. This is consistent with a defective hypoxic response. Similarly, women with HMB did not have the increase in HIF-1α downstream targets at menstruation that was seen in those with normal bleeding. Women with HMB bled for 2 additional days, consistent with delayed endometrial repair.
To define the role of endometrial hypoxia, we prevented its occurrence in our mouse simulated menses model, by placing mice in hyperoxia (75% O2) during menstruation. This resulted in reduced endometrial HIF-1α and delayed endometrial repair. HIF-1α heterozygote mice are phenotypically normal, but are unable to mount an appropriate HIF-1 response in hypoxia. Simulation of menses in these mice also resulted in significantly delayed endometrial repair.
As our human studies suggest that women with HMB have a defective hypoxic response in their endometrium during menses, we utilised our mouse model of non-hypoxic menstruation to investigate novel therapeutic strategies. Dimethyloxyglycine (DMOG) is a pharmacological agent that stabilises HIF-1α, even in the presence of oxygen. DMOG administration during menstruation restored normal endometrial repair.
CONCLUSIONS
This study reveals for the first time that hypoxia is required during menstruation to optimise endometrial repair. Increasing HIF-1 at menses shows real promise as a novel, non-hormonal medical treatment to limit menstrual blood loss.
Jackie Maybin, MRC Centre for Reproductive Health, University of Edinburgh
This research has been published as Maybin JA et al. 2018 Nature Communications doi:10.1038/s41467-017-02375-6.
REFERENCES
- Maybin JA et al. 2018 Nature Communications doi:10.1038/s41467-017-02375-6.
- Markee JE 1940 Contributions to Embryology 177 220–230.
- Zhang J & Salamonsen LA 2002 Human Reproduction 17 265–274.
- Gaide Chevronnay HP et al. 2010 Endocrinology 151 4515–4526.
- Coudyzer P et al. 2013 FASEB Journal 27 3711–3719.



{kind=link}