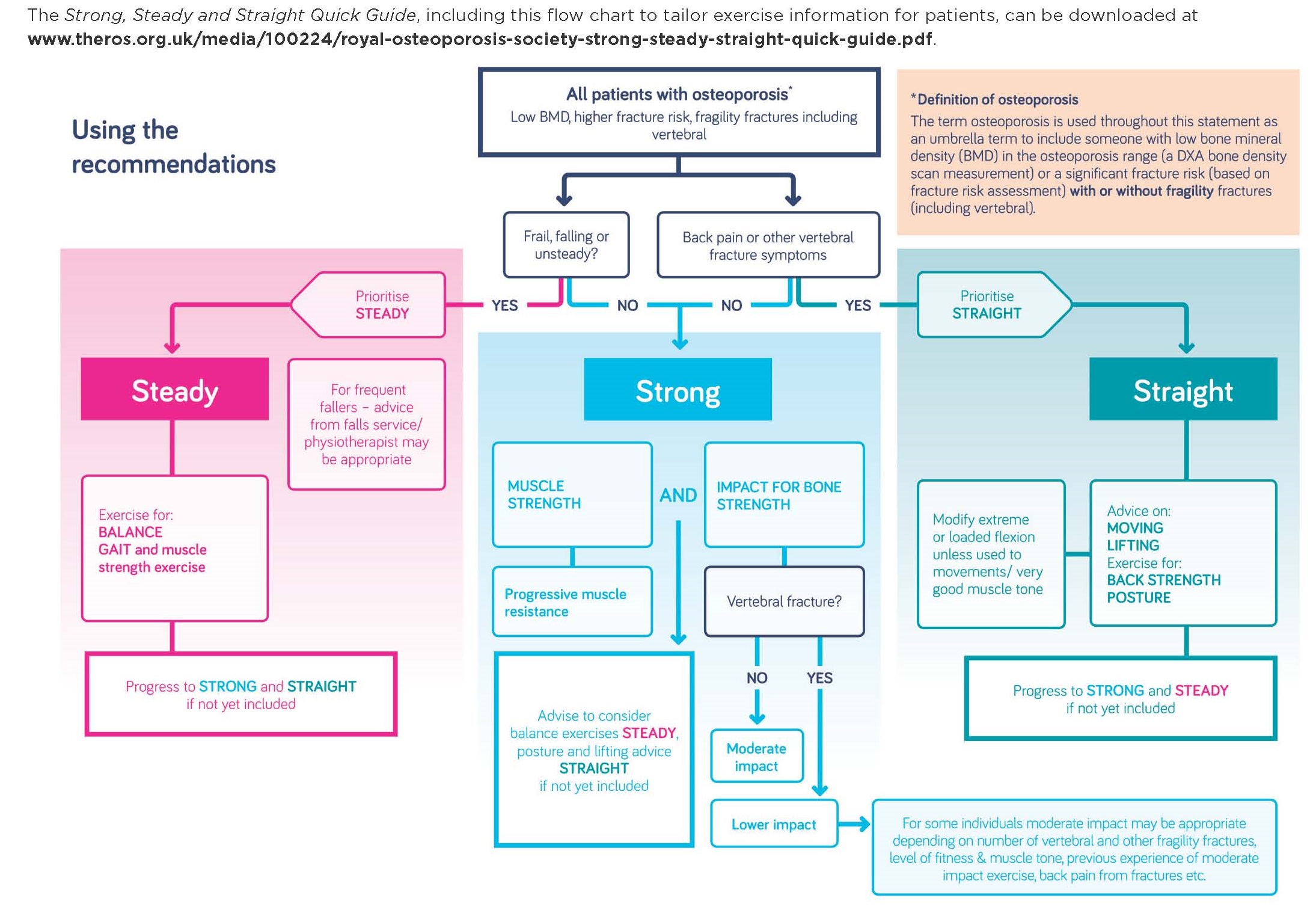
The Royal Osteoporosis Society (with support from organisations such as the Society for Endocrinology) has worked with scientists and clinicians in the field of osteoporosis and bone health to produce a consensus statement1 on the role of physical activity and exercise for osteoporosis, with new information resources for patients.2 This publication will help clinicians advise their patients with osteoporosis more appropriately and confidently. New information clarifies the types of exercise that will help patients optimise their bone health and reduce their risk of fragility fractures.
WHY A CONSENSUS STATEMENT?
Patients with osteoporosis often ask what exercise they should do to reduce their risk of fracture, and how safe this is. We frequently encourage weightbearing exercise, while discouraging bending forward, to reduce the risk of vertebral fractures. If we are honest, we aren’t too secure or confident in our response, and patients have probably gone away somewhat confused and maybe fearful about what they should and shouldn’t do.
Royal Osteoporosis Society helpline reports, surveys and stakeholder group meetings not only confirmed that these experiences were common, but also found, worryingly, that patients often do less exercise and activity after their osteoporosis ‘diagnosis’.3–5
This uncertainty and confusion about the effectiveness and safety of physical activity and exercise in promoting bone strength and reducing fracture risk in patients with osteoporosis prompted the Royal Osteoporosis Society to produce a consensus statement. The aim was to improve professionals’ knowledge and practice and, consequently, the care and advice received by patients.
DEVELOPING THE STATEMENT
Experts, including scientists, academics, health and exercise professionals, and patient representatives were invited to examine the evidence and commission further evidence reviews. Since comprehensive evidence reviews had recently been completed,6–8 a further systematic review was not felt necessary. Instead, a review was commissioned to ‘fill the gaps’, especially in relation to ‘exercise harms’.9 The group aimed to reach an expert consensus in those frequent instances where evidence was limited, with the intention of making positive recommendations where potential benefits were considered to outweigh harms.
THEMES AND RECOMMENDATIONS
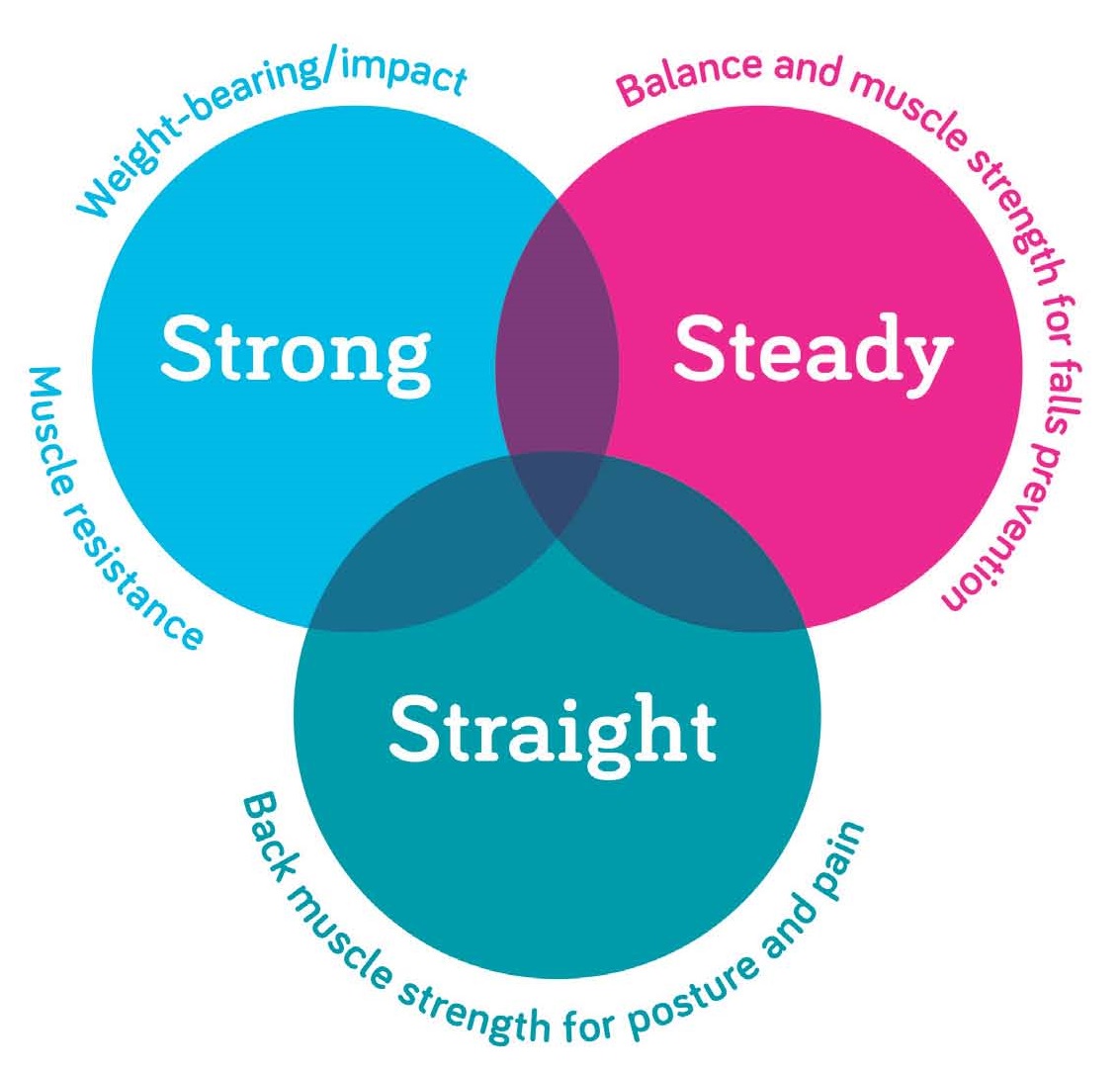
The consensus statement identifies three themes under which being physically active and taking exercise can help with osteoporosis.
STRONG
Exercise to promote bone and muscle strength
This advice should be integrated with the Chief Medical Officers’ recommendations on physical activity for general health.10 The statement also cautions that exercise should not be a replacement for pharmacological interventions to reduce fracture risk.
Recommendations:
- Weight-bearing exercise with impact (standing up and moving with some added force) is recommended as follows. About 50 moderate impacts, such as jogs or low level jumps, should be undertaken on most days. For patients with vertebral or multiple other fractures, or for those who are less able, 20 mins of lower impact exercise, such as walking or marching, is recommended. A variety of activities or exercises involving different directions, movements and speeds is ideal. For those who are frail or less able to exercise then, at least, reducing prolonged periods of ‘sitting’ is recommended (e.g. standing up for a minute or two every hour).
- Gradually increase the intensity of the muscle resistance exercise. Consider using weights or elastic resistance bands and build up to three sets of 8–12 ‘repetitions max’ (the most you can lift 8–12 times), as part of an exercise programme or activity that works on all the main muscle groups in the body. Advice from a gym or exercise instructor may be necessary in the case of some types of exercise, to ensure safe and effective techniques.
Evidence: There is evidence that being physically active is associated with a reduction in hip fracture risk11 (this may partly be mediated by a reduction in falls risk) and that exercise maintains bone strength, reduces loss of bone mineral density (BMD) and promotes bone strength.6,8,12,13
In terms of the populations that may benefit from exercise interventions, there is some evidence that exercise improves BMD in post-menopausal women.12 However, more research is needed in older people, especially those with reduced bone strength.6 Some recent research has focused on specific types of exercise, such as moderate impact and high intensity muscle resistance exercise undertaken by older women, which led to improvements in BMD.14
STEADY
Exercise and activity to promote steadiness, so preventing falls and reducing fall-related fractures
Recommendations:
- Balance and muscle-strengthening exercises are recommended for those over 65 years, or anyone with balance problems, especially before they start new challenging physical activity, such as brisk walking.
- If patients are already falling, then a referral to a falls service or physiotherapist for a multifactorial falls risk assessment and advice should also be considered.
Evidence: There is good evidence that exercise and physical activity reduce the risk of falls. Most non-vertebral fragility fractures are caused by falls and, in principle, reducing falls risk is likely to reduce fractures. However, more research is needed to confirm that exercise interventions reduce the falls that result in fractures.15
STRAIGHT
Back-strengthening exercise and safe moving and lifting, to reduce the risk of vertebral fractures and help improve associated symptoms
Though applicable to all patients with osteoporosis, specific recommendations need to be tailored to the individual, taking personal preferences into account.
Recommendations:
- Consider modifying or finding alternatives to exercises or movements that involve sustained, end range or loaded forward flexion such as ‘sit ups’ or the ‘roll down’ in pilates. This is especially important for those without strong abdominal muscle strength, or those who find movements difficult or uncomfortable. These movements have the potential to put increased force or pressure on the anterior vertebral bodies and may increase fracture risk.
- Back-strengthening exercises are recommended on 2–3 days per week, to help with posture and prevent pain after vertebral fractures (or daily to help with existing pain).
- Patients with painful vertebral fracture need prompt advice to reduce anxiety levels. They may benefit from a referral to a physiotherapist for a tailored exercise programme. Evidence: There is some evidence to suggest that exercise may help to improve symptoms16 and quality of life17 after painful vertebral fractures.
There is considerable evidence and recognition10 that physical activity and exercise are important for general health as well as bone health. If people diagnosed with osteoporosis reduce their physical activity because of fears of causing a fracture, this may cause other poor health outcomes.
SAFETY
The consensus statement supports participation in moderate impact exercise, such as jogging and low level jumping, to promote bone strength in patients with osteoporosis. So long as exercise is built up gradually, the risk that this will lead to a vertebral fracture is negligible. Similarly, using weights, even after vertebral fractures, can be useful for improving bone and muscle strength, though it’s important that these are tailored to the individual, and that patients are taught good techniques. No specific weight limits or restrictions are recommended.
A more cautious approach is recommended if patients have had vertebral fractures or multiple other fragility fractures, or if they have had a fracture in relation to impact exercise. However, there is no absolute contraindication to moderate impact exercise for these patients. The statement recognises that it may be appropriate for these patients to gradually build up to moderate impact exercise, particularly for those already used to this type of exercise.
Recommendations for safe moving and lifting are based on a principle of ‘good preventative measures for all’. They propose that everyone with osteoporosis should learn to ‘hip hinge’ for safe lifting and moving. Similarly, alternatives or modifications to some types of movement and exercises in pilates, yoga and related activities are recommended.
Generally, a ‘how to’, positive and encouraging approach by professionals to exercise and physical activity is strongly recommended, both to increase appropriate exercise for fracture risk reduction and management, and to maintain activity for general health.
Sarah Leyland, Nurse Consultant, Royal Osteoporosis Society
Jon Tobias, Professor in Rheumatology, University of Bristol; Honorary Consultant North Bristol NHS Trust
REFERENCES
- Royal Osteoporosis Society 2018 Strong, Steady and Straight www.theros.org.uk/strong-steady-and-straight.
- Royal Osteoporosis Society 2019 Exercise and Physical Activity for Osteoporosis and Bone Health www.theros.org.uk/exercise.
- Paskins Z 2017 Views on Strong, Straight and Steady Project: Findings from Stakeholder Advisory Groups with Public and Professionals. Bath: National Osteoporosis Society.
- Clark R 2017 Strong, Straight and Steady Survey Report. Bath: National Osteoporosis Society.
- Reventlow SD 2007 Scandinavian Journal of Primary Health Care 25 160–165.
- Giangregorio LM et al. 2014 Osteoporosis International 25 821–835.
- Giangregorio LM et al. 2015 Osteoporosis International 26 891–910.
- Beck BR et al. 2017 Journal of Science & Medicine in Sport 20 438–445.
- Knutsnor S et al. 2018 Journal of Frailty, Sarcopenia & Falls 3 155–178.
- UK Chief Medical Officers 2011 Start Active, Stay Active www.gov.uk/government/publications/start-active-stay-active-a-report-on-physical-activity-from-the-four-home-countries-chief-medical-officers.
- Gregg EW et al. 2000 Journal of the American Geriatrics Society 48 883–893.
- Howe TE et al. 2011 Cochrane Database of Systematic Reviews doi: 10.1002/14651858.CD000333.pub2.
- Kohrt WM et al. 2004 Medicine & Science in Sports & Exercise 36 1985–1996.
- Watson SL et al. 2017 Journal of Bone & Mineral Research 33 211–220.
- Sherrington C et al. 2019 Cochrane Database of Systematic Reviews doi: 10.1002/14651858.CD012424.pub2.
- Giangregorio LM et al. 2013 Cochrane Database of Systematic Reviews doi: 10.1002/14651858.CD008618.pub2.
- Kanemaru A et al. 2010 Archives of Gerontology & Geriatrics 51 169–172.



{kind=link}
{kind=link}